

Determination of MIC Breakpoints for Second-Line Drugs Associated with Clinical Outcomes in Multidrug-Resistant Tuberculosis Treatment in China
- PMID: 27246779
- PMCID: PMC4958164
- DOI: 10.1128/AAC.03008-15
Determination of MIC Breakpoints for Second-Line Drugs Associated with Clinical Outcomes in Multidrug-Resistant Tuberculosis Treatment in China
Abstract
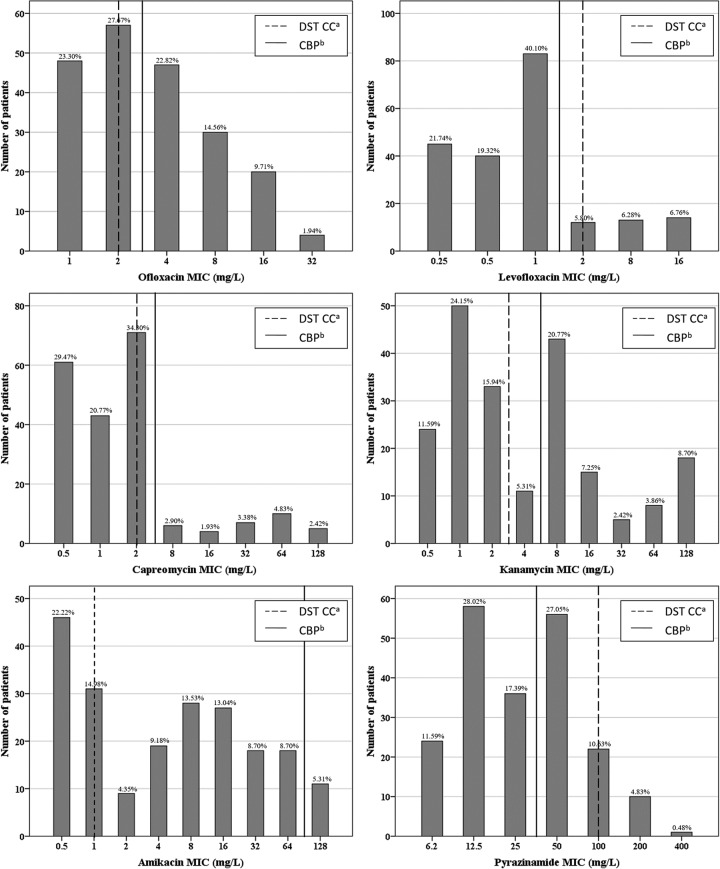
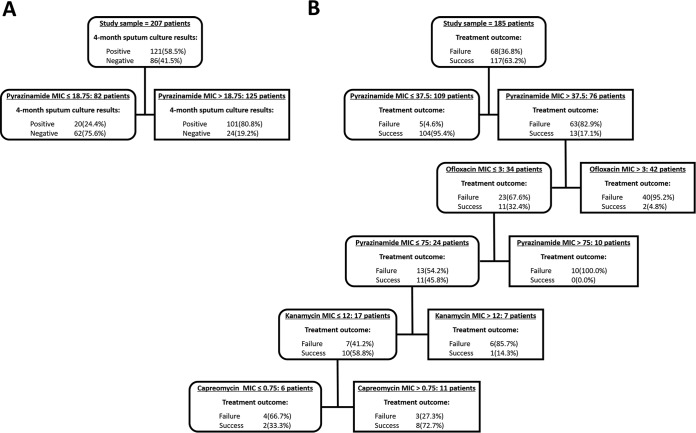
Our study aims to identify the clinical breakpoints (CBPs) of second-line drugs (SLDs) above which standard therapy fails in order to improve multidrug-resistant tuberculosis (MDR-TB) treatment. MICs of SLDs were determined for M. tuberculosis isolates cultured from 207 MDR-TB patients in a prospective cohort study in China between January 2010 and December 2012. Classification and regression tree (CART) analysis was used to identify the CBPs predictive of treatment outcome. Of the 207 MDR-TB isolates included in the present study, the proportion of isolates above the critical concentration recommended by WHO ranged from 5.3% in pyrazinamide to 62.8% in amikacin. By selecting pyrazinamide as the primary node (CBP, 18.75 mg/liter), 72.1% of sputum culture conversions at month four could be predicted. As for treatment outcome, pyrazinamide (CBP, 37.5 mg/liter) was selected as the primary node to predict 89% of the treatment success, followed by ofloxacin (CBP, 3 mg/liter), improving the predictive capacity of the primary node by 10.6%. Adjusted by identified confounders, the CART-derived pyrazinamide CBP remained the strongest predictor in the model of treatment outcome. Our findings indicate that the critical breakpoints of some second-line drugs and PZA need to be reconsidered in order to better indicate MDR-TB treatment outcome.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Bastos ML, Hussain H, Weyer K, Garcia-Garcia L, Leimane V, Leung CC, Narita M, Pena JM, Ponce-de-Leon A, Seung KJ, Shean K, Sifuentes-Osornio J, Van der Walt M, Van der Werf TS, Yew WW, Menzies D, Collaborative Group for Meta-Analysis of Individual Patient Data in MDR-TB. 2014. Treatment outcomes of patients with multidrug-resistant and extensively drug-resistant tuberculosis according to drug susceptibility testing to first- and second-line drugs: an individual patient data meta-analysis. Clin Infect Dis 59:1364–1374. doi: 10.1093/cid/ciu619. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
