

Systematic Review and Meta-analysis of Clinical and Economic Outcomes from the Implementation of Hospital-Based Antimicrobial Stewardship Programs
- PMID: 27246783
- PMCID: PMC4958232
- DOI: 10.1128/AAC.00825-16
Systematic Review and Meta-analysis of Clinical and Economic Outcomes from the Implementation of Hospital-Based Antimicrobial Stewardship Programs
Abstract
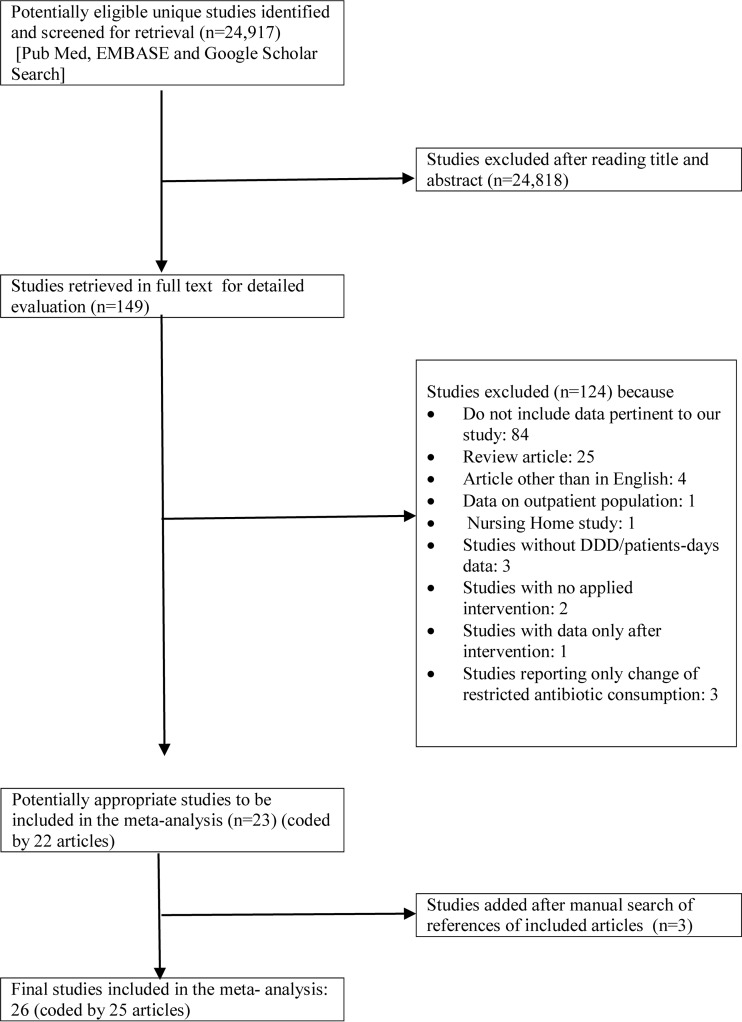
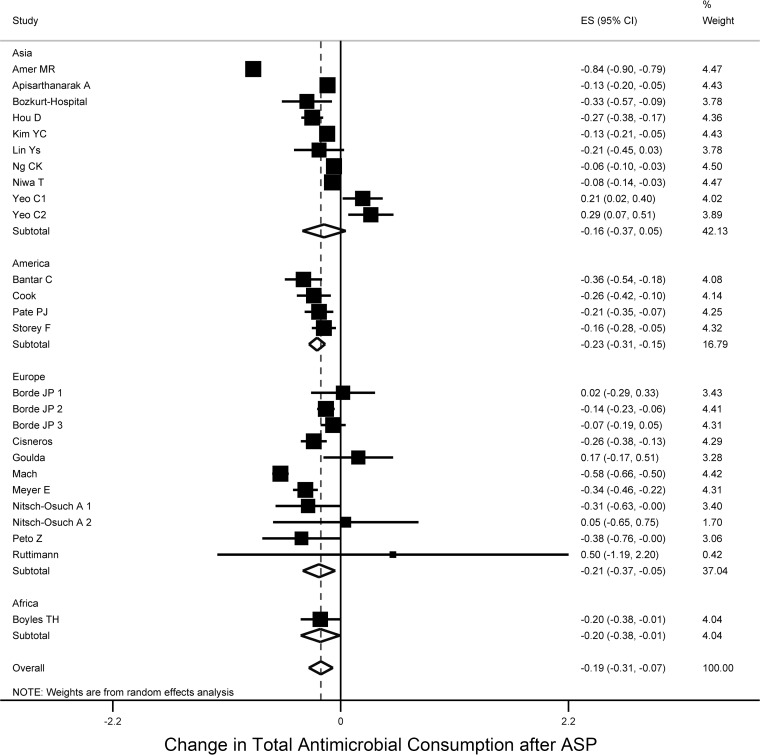
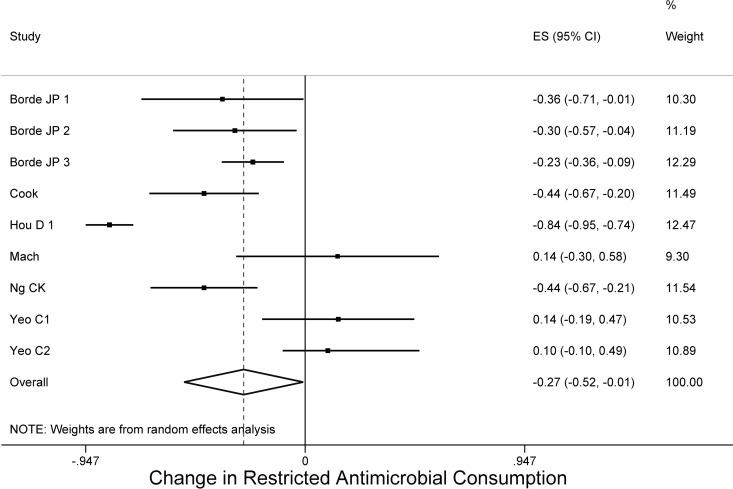
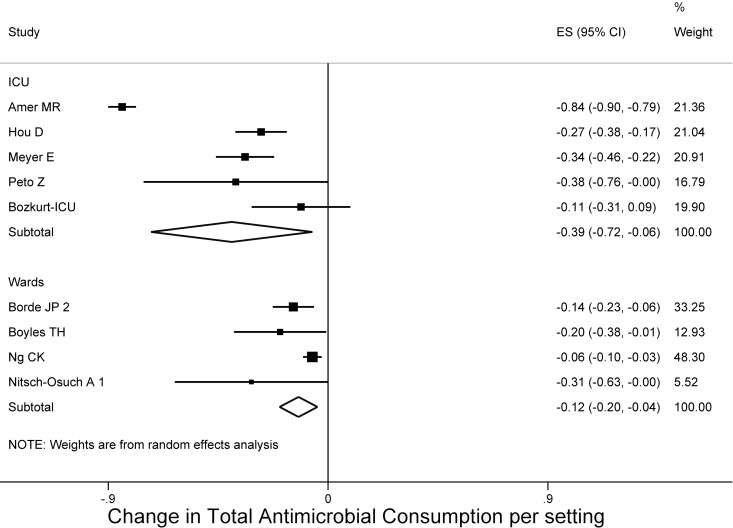
The implementation of antimicrobial stewardship programs (ASPs) is a promising strategy to help address the problem of antimicrobial resistance. We sought to determine the efficacy of ASPs and their effect on clinical and economic parameters. We searched PubMed, EMBASE, and Google Scholar looking for studies on the efficacy of ASPs in hospitals. Based on 26 studies (extracted from 24,917 citations) with pre- and postimplementation periods from 6 months to 3 years, the pooled percentage change of total antimicrobial consumption after the implementation of ASPs was -19.1% (95% confidence interval [CI] = -30.1 to -7.5), and the use of restricted antimicrobial agents decreased by -26.6% (95% CI = -52.3 to -0.8). Interestingly, in intensive care units, the decrease in antimicrobial consumption was -39.5% (95% CI = -72.5 to -6.4). The use of broad-spectrum antibiotics (-18.5% [95% CI = -32 to -5.0] for carbapenems and -14.7% [95% CI = -27.7 to -1.7] for glycopeptides), the overall antimicrobial cost (-33.9% [95% CI = -42.0 to -25.9]), and the hospital length of stay (-8.9% [95% CI = -12.8 to -5]) decreased. Among hospital pathogens, the implementation of ASPs was associated with a decrease in infections due to methicillin-resistant Staphylococcus aureus (risk difference [RD] = -0.017 [95% CI = -0.029 to -0.005]), imipenem-resistant Pseudomonas aeruginosa (RD = -0.079 [95% CI = -0.114 to -0.040]), and extended-spectrum beta-lactamase Klebsiella spp. (RD = -0.104 [95% CI = -0.153 to -0.055]). Notably, these improvements were not associated with adverse outcomes, since the all-cause, infection-related 30-day mortality and infection rates were not significantly different after implementation of an ASP (RD = -0.001 [95% CI = -0.009 to 0.006], RD = -0.005 [95% CI = -0.016 to 0.007], and RD = -0.045% [95% CI = -0.241 to 0.150], respectively). Hospital ASPs result in significant decreases in antimicrobial consumption and cost, and the benefit is higher in the critical care setting. Infections due to specific antimicrobial-resistant pathogens and the overall hospital length of stay are improved as well. Future studies should focus on the sustainability of these outcomes and evaluate potential beneficial long-term effects of ASPs in mortality and infection rates.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures


References
-
- Fridkin SK, Steward CD, Edwards JR, Pryor ER, McGowan JE Jr, Archibald LK, Gaynes RP, Tenover FC. 1999. Surveillance of antimicrobial use and antimicrobial resistance in United States hospitals: project ICARE phase 2. Project Intensive Care Antimicrobial Resistance Epidemiology (ICARE) hospitals. Clin Infect Dis 29:245–252. - PubMed
-
- Centers for Disease Control and Prevention. 2013. Antibiotic resistance threats in the United States, 2013. Centers for Disease Control and Prevention, Atlanta, GA: http://www.cdc.gov/drugresistance/threat-report-2013/.
-
- Dellit TH, Owens RC, McGowan JE Jr, Gerding DN, Weinstein RA, Burke JP, Huskins WC, Paterson DL, Fishman NO, Carpenter CF, Brennan PJ, Billeter M, Hooton TM. 2007. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis 44:159–177. doi: 10.1086/510393. - DOI - PubMed
-
- Fridkin SK, Baggs J, Fagan R, Magill S, Pollack LA, Malpiedi P, Slayton R, Khader K, Rubin MA, Jones M, Samore MH, Dumyati G, Dodds-Ashley E, Meek J, Yousey-Hindes K, Jernigan J, Shehab N, Herrera R, McDonald LC, Schneider A, Srinivasan A. 2014. Vital signs: improving antibiotic use among hospitalized patients. MMWR Morb Mortal Wkly Rep 63:194–200. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
