

Clinical characterisation and phylogeny of respiratory syncytial virus infection in hospitalised children at Red Cross War Memorial Children's Hospital, Cape Town
- PMID: 27246848
- PMCID: PMC4888648
- DOI: 10.1186/s12879-016-1572-5
Clinical characterisation and phylogeny of respiratory syncytial virus infection in hospitalised children at Red Cross War Memorial Children's Hospital, Cape Town
Abstract
Background: Respiratory syncytial virus (RSV) is a major cause of lower respiratory tract infection in young children in both the community and hospital setting.
Methods: The clinical presentation, patient and phylogenetic characteristicsof laboratory-confirmed cases of RSV, as well as risk factors for nosocomial infectionat Red Cross War Memorial Children's Hospital in Cape Town were analysed. A multiplex PCR assay that detects 7 respiratory viruses was used to identify RSV nucleic acid on respiratory specimens.
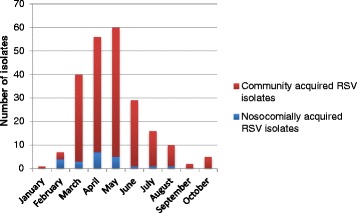
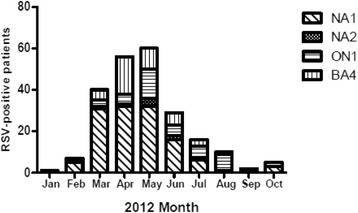
Results: A total of 226 children were studied, ages ranging between 1 week and 92.5 months (median: 2.8 months, IQR: 1.3-6.3 months) and 51.8 % were males. The median duration of symptoms prior to diagnosis was 2 days (IQR: 1-4 days). Nosocomial infections wereidentified in 22 (9.7 %) children. There were pre-existing medical conditions in 113 (50.0 %) excluding HIV, most commonly prematurity (n = 58, 50.0 %) and congenital heart disease (n = 34, 29.3 %). The commonest presenting symptoms were cough (196, 86.7 %), difficulty in breathing (115, 50.9 %) and fever (91, 41.6 %).A case fatality rate of 0.9 % was recorded. RSV group A predominated (n = 181, 80.1 %) while group B accounted for only 45 (19.9 %) of the infections. The prevalent genotypes were NA1 (n = 127,70.1 %), ON1 (n = 45,24.9 %) and NA2 (n = 9,5.0 %) for group A while the only circulating RSV B genotype was BA4. There was no significant difference in the genotype distribution between the nosocomial and community-acquired RSV infections. Age ≥ 6 months was independently associated with nosocomial infection.
Conclusions: A large percentage of children with RSV infection had pre-existing conditions. Approximately one tenth of the infections were nosocomial with age 6 months or older being a risk factor. Though both RSV groups co-circulated during the season, group A was predominant and included the novel ON1 genotype. Continued surveillance is necessary to identify prevalent and newly emerging genotypes ahead of vaccine development and efficacy studies.
Keywords: Clinical characteristics; Genetic diversity; Nosocomial infection; Respiratory syncytial virus.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
