

Safety and efficacy of ruxolitinib in an open-label, multicenter, single-arm phase 3b expanded-access study in patients with myelofibrosis: a snapshot of 1144 patients in the JUMP trial
- PMID: 27247324
- PMCID: PMC5060023
- DOI: 10.3324/haematol.2016.143677
Safety and efficacy of ruxolitinib in an open-label, multicenter, single-arm phase 3b expanded-access study in patients with myelofibrosis: a snapshot of 1144 patients in the JUMP trial
Abstract
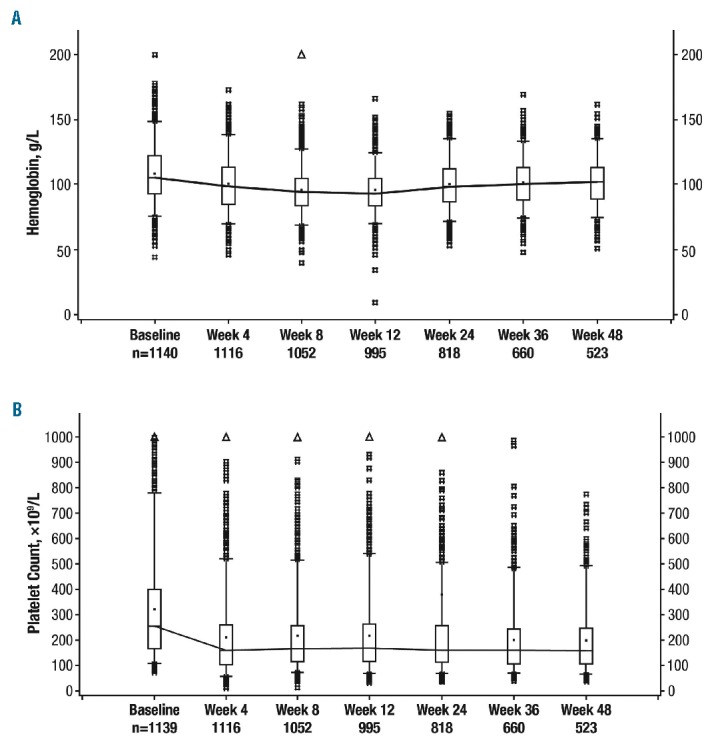
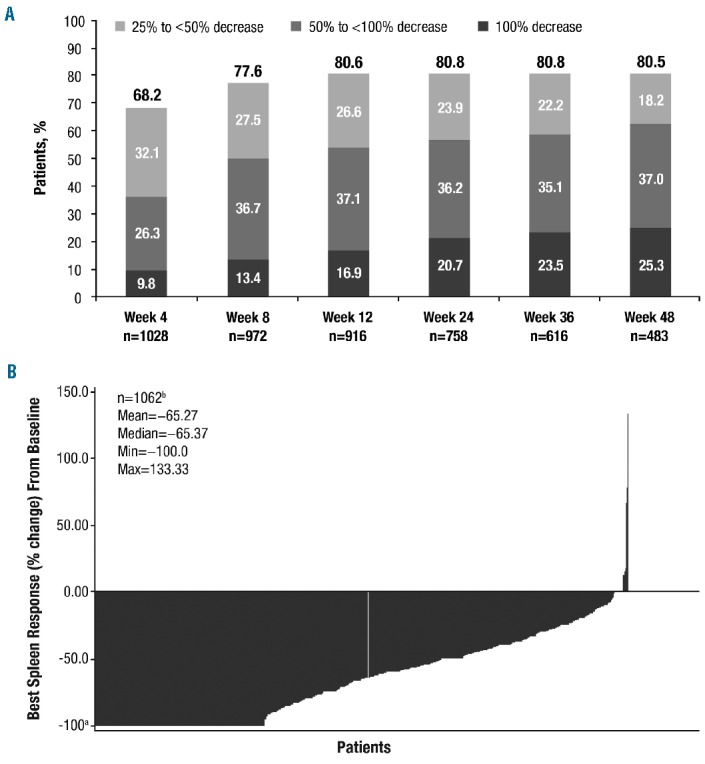
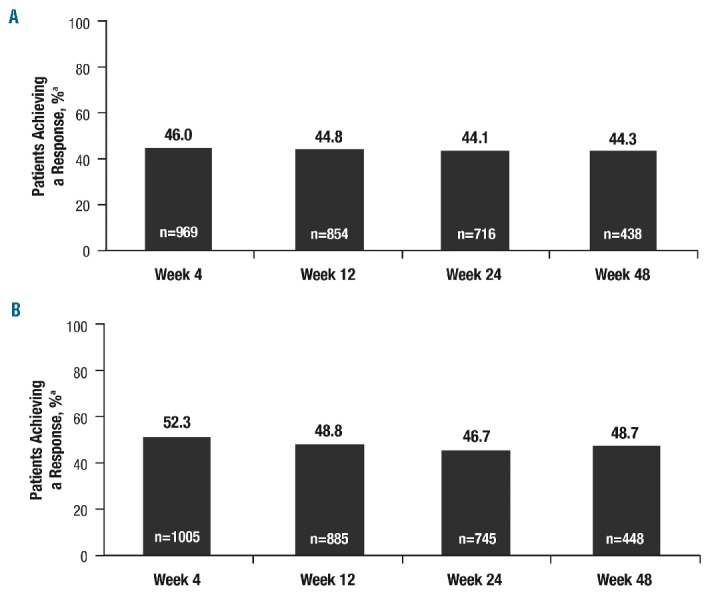
JUMP is a phase 3b expanded-access trial for patients without access to ruxolitinib outside of a clinical study; it is the largest clinical trial to date in patients with myelofibrosis who have been treated with ruxolitinib. Here, we present safety and efficacy findings from an analysis of 1144 patients with intermediate- or high-risk myelofibrosis, as well as a separate analysis of 163 patients with intermediate-1-risk myelofibrosis - a population of patients not included in the phase 3 COMFORT studies. Consistent with ruxolitinib's mechanism of action, the most common hematologic adverse events were anemia and thrombocytopenia, but these led to treatment discontinuation in only a few cases. The most common non-hematologic adverse events were primarily grade 1/2 and included diarrhea, pyrexia, fatigue, and asthenia. The rates of infections were low and primarily grade 1/2, and no new or unexpected infections were observed. The majority of patients achieved a ≥50% reduction from baseline in palpable spleen length. Improvements in symptoms were rapid, with approximately half of all patients experiencing clinically significant improvements, as assessed by various quality-of-life questionnaires. The safety and efficacy profile in intermediate-1-risk patients was consistent with that in the overall JUMP population and with that previously reported in intermediate-2- and high-risk patients. Overall, ruxolitinib provided clinically meaningful reductions in spleen length and symptoms in patients with myelofibrosis, including those with intermediate-1-risk disease, with a safety and efficacy profile consistent with that observed in the phase 3 COMFORT studies. This trial was registered as NCT01493414 at ClinicalTrials.gov.
Copyright© Ferrata Storti Foundation.
Figures
References
-
- Mesa RA, Verstovsek S, Cervantes F, et al. Primary myelofibrosis (PMF), post polycythemia vera myelofibrosis (post-PV MF), post essential thrombocythemia myelofibrosis (post-ET MF), blast phase PMF (PMF-BP): consensus on terminology by the International Working Group for Myelofibrosis Research and Treatment (IWG-MRT). Leuk Res. 2007;31(6):737–740. - PubMed
-
- Swerdlow SH, Campo E, Harrison NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Vol 2 4th ed. Geneva, Switzerland: World Health Organization; 2008.
-
- Vardiman JW, Thiele J, Arber DA, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood. 2009;114(5):937–951. - PubMed
-
- Tefferi A. Primary myelofibrosis: 2013 update on diagnosis, risk-stratification, and management. Am J Hematol. 2013;88(2): 141–150. - PubMed
-
- Mesa RA, Niblack J, Wadleigh M, et al. The burden of fatigue and quality of life in myeloproliferative disorders (MPDs): an international Internet-based survey of 1179 MPD patients. Cancer. 2007;109(1):68–76. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
