

Radiological interventions in malignant biliary obstruction
- PMID: 27247718
- PMCID: PMC4882409
- DOI: 10.4329/wjr.v8.i5.518
Radiological interventions in malignant biliary obstruction
Abstract
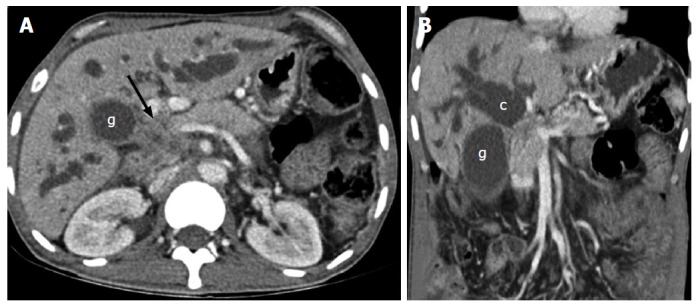
Malignant biliary obstruction is commonly caused by gall bladder carcinoma, cholangiocarcinoma and metastatic nodes. Percutaneous interventions play an important role in managing these patients. Biliary drainage, which forms the major bulk of radiological interventions, can be palliative in inoperable patients or pre-operative to improve liver function prior to surgery. Other interventions include cholecystostomy and radiofrequency ablation. We present here the indications, contraindications, technique and complications of the radiological interventions performed in patients with malignant biliary obstruction.
Keywords: Biliary drainage; Biliary interventions; Biliary malignancy; Biliary obstruction; Cholecystostomy; Interventional radiology.
Figures
Similar articles
-
Indian College of Radiology and Imaging Evidence-Based Guidelines for Percutaneous Image-Guided Biliary Procedures.Indian J Radiol Imaging. 2021 Apr;31(2):421-440. doi: 10.1055/s-0041-1734222. Epub 2021 Jul 28. Indian J Radiol Imaging. 2021. PMID: 34556927 Free PMC article. Review.
-
[Percutaneous biliary and gallbladder interventions].Radiologe. 2019 Apr;59(4):342-347. doi: 10.1007/s00117-019-0506-9. Radiologe. 2019. PMID: 30806733 Review. German.
-
Current interventional options for palliative care for patients with advanced-stage cholangiocarcinoma.World J Clin Oncol. 2024 Mar 24;15(3):381-390. doi: 10.5306/wjco.v15.i3.381. World J Clin Oncol. 2024. PMID: 38576598 Free PMC article. Review.
-
Role of radiofrequency ablation in advanced malignant hilar biliary obstruction.Clin Endosc. 2023 Mar;56(2):155-163. doi: 10.5946/ce.2022.218. Epub 2023 Jan 16. Clin Endosc. 2023. PMID: 36646424 Free PMC article. Review.
-
Interventional radiofrequency ablation: A promising therapeutic modality in the management of malignant biliary and pancreatic duct obstruction.J Cancer. 2018 Jan 5;9(4):629-637. doi: 10.7150/jca.23280. eCollection 2018. J Cancer. 2018. PMID: 29556320 Free PMC article.
Cited by
-
Therapeutic EUS: Biliary drainage - The interventional radiologist's perspective.Endosc Ultrasound. 2017 Dec;6(Suppl 3):S127-S131. doi: 10.4103/eus.eus_77_17. Endosc Ultrasound. 2017. PMID: 29387709 Free PMC article. No abstract available.
-
Diagnostic accuracy of ultrasonography in adults with obstructive jaundice.J Ultrason. 2020;20(81):e100-e105. doi: 10.15557/JoU.2020.0016. Epub 2020 Jun 15. J Ultrason. 2020. PMID: 32609962 Free PMC article.
-
Indian College of Radiology and Imaging Evidence-Based Guidelines for Percutaneous Image-Guided Biliary Procedures.Indian J Radiol Imaging. 2021 Apr;31(2):421-440. doi: 10.1055/s-0041-1734222. Epub 2021 Jul 28. Indian J Radiol Imaging. 2021. PMID: 34556927 Free PMC article. Review.
-
Total Fluoroscopy Time Reduction During Ultrasound- and Fluoroscopy-Guided Percutaneous Transhepatic Biliary Drainage Procedure: Importance of Adjusting the Puncture Angle.Med Sci Monit. 2021 Nov 21;27:e933889. doi: 10.12659/MSM.933889. Med Sci Monit. 2021. PMID: 34802031 Free PMC article.
-
Is Palliative Percutaneous Drainage for Malignant Biliary Obstruction Useful?World J Surg. 2018 Sep;42(9):2980-2986. doi: 10.1007/s00268-018-4567-0. World J Surg. 2018. PMID: 29536143
References
-
- van Delden OM, Laméris JS. Percutaneous drainage and stenting for palliation of malignant bile duct obstruction. Eur Radiol. 2008;18:448–456. - PubMed
-
- Taylor MC, McLeod RS, Langer B. Biliary stenting versus bypass surgery for the palliation of malignant distal bile duct obstruction: a meta-analysis. Liver Transpl. 2000;6:302–308. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
