

Causes and factors related to dopamine agonist withdrawal in Parkinson's disease
- PMID: 27247848
- PMCID: PMC4864043
- DOI: 10.1002/brb3.453
Causes and factors related to dopamine agonist withdrawal in Parkinson's disease
Abstract
Background: Although dopamine agonists (DAs) are useful in Parkinson's disease (PD), they are not frequently used in elderly patients due to adverse effects. However, there is a lack of evidence because few elderly PD patients are enrolled in clinical trials.
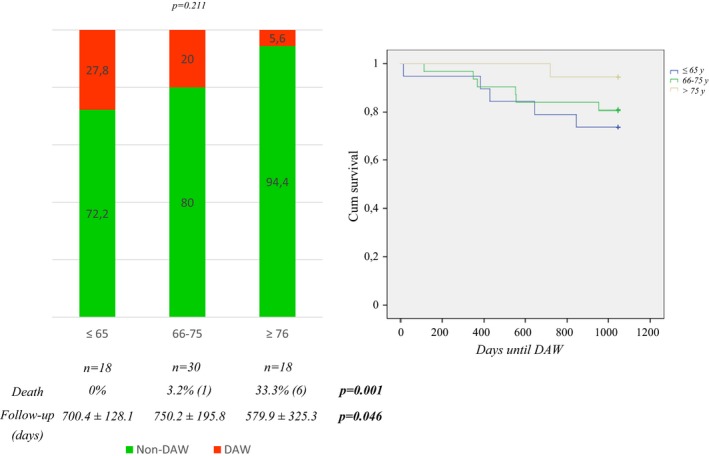
Aims of the study: The aims of this study were to analyze the reasons of DA withdrawal (DAW) in a group of PD patients in clinical practice and to identify the related factors. Specifically, we studied the effect of age, comorbidity, and polypharmacy as potential risk factors for DAW.
Methods: A retrospective chart review of the follow-up (from May, 2012 to March, 2015) of a subgroup of PD patients receiving a DA (n = 68; 60.3% males, 69.3 ± 9.2 years old) from a cohort (n = 150) previously studied in detail in 2012 was used to identify predictive factors of DAW.
Results: The DAW percentage was 18.2% (12/66; follow-up of 690.2 ± 232.6 days). DAW causes were cognitive impairment (3), reduction therapy (3), hallucinations (2), dyskinesia (2), and excessive diurnal somnolence (2). Only a higher levodopa daily dose (HR 1.003; 95% CI 1.001-1.006; P = 0.044) was an independent predictor of DAW after adjustment for other explanatory variables.
Conclusions: The frequency of DAW was low. Advanced age alone is not a contraindication to the administration of DAs.
Keywords: Age; Parkinson′s disease; comorbidity; dopamine agonist; polypharmacy; tolerability.
Figures


References
-
- Antonini, A. , Tolosa E., Mizuno Y., Yamamoto M., and Poewe W. H.. 2009. A reassessment of risk and benefits of dopamine agonists in Parkinson′s disease. Lancet Neurol. 8:929–937. - PubMed
-
- Arbouw, M. E. , van Vugt J. P., Egberts T. C., and Guchelaar H. J.. 2007. Pharmacogenetics of antiparkinsonian drug treatment: a systematic review. Pharmacogenomics 8:159–176. - PubMed
-
- Arbouw, M. E. , Movig K. L., Guchejaar H. J., Poels P. J., van Vugt J. P., Neef C., et al. 2008. Discontinuation of ropinirole and pramipexole in patients with Parkinson's disease in clinical practice versus clinical trials. Eur. J. Clin. Pharmacol. 64:1021–1026. - PubMed
-
- Biglan, K. M. , Holloway R. G. Jr, McDermott M. P., Richard I. H., and Parkinson Study Group CALM‐PD Investigators . 2007. Risk factors for somnolence, edema, and hallucinations in early Parkinson disease. Neurology 69:187–195. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
