

Resolution of Chronic Aspiration Pneumonitis Following Endoscopic Endonasal Repair of Spontaneous Cerebrospinal Fluid Fistula of the Skull Base
- PMID: 27247911
- PMCID: PMC4870059
- DOI: 10.1055/s-0036-1582238
Resolution of Chronic Aspiration Pneumonitis Following Endoscopic Endonasal Repair of Spontaneous Cerebrospinal Fluid Fistula of the Skull Base
Abstract
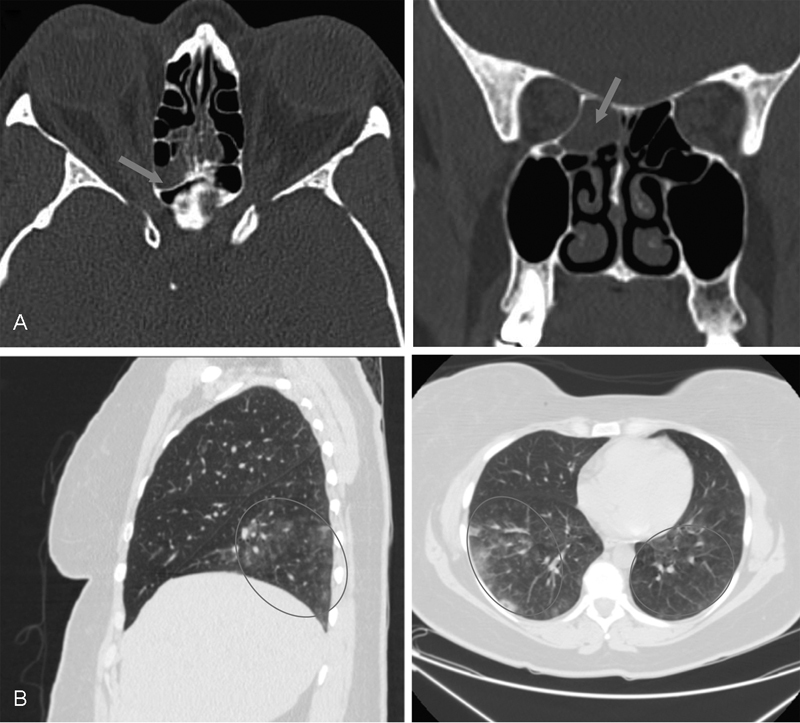
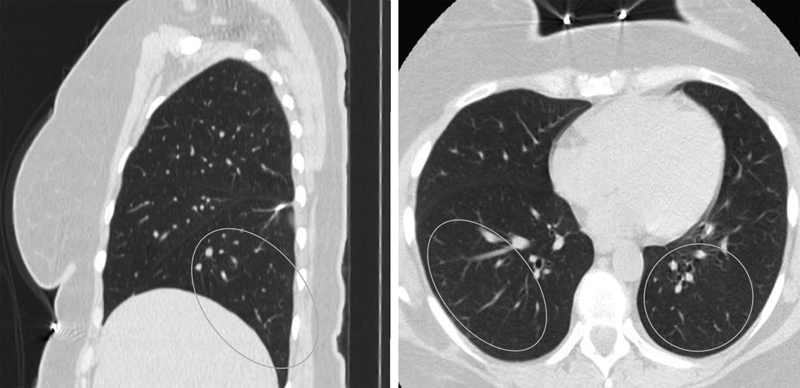
Spontaneous cerebrospinal fluid (CSF) rhinorrhea due to a skull base defect requires prompt diagnosis and treatment. Multiple surgical options are available for repairing the fistula, including the two-layer "fascial apposition" method and use of a pedicled nasal-septal flap. A 44-year-old obese woman presented with 4 months of progressive cough, exertional dyspnea, hoarseness, and intermittent fluid drainage from the right nostril. Chest computed tomography (CT) imaging and bronchoscopy showed chronic pneumonitis, which was confirmed by pulmonary wedge resection. CT and magnetic resonance imaging of the skull base, as well as laboratory analysis of the nasal fluid for β2-transferrin, confirmed a skull base defect causing CSF rhinorrhea. During surgery, insertion of a lumbar drain with the intrathecal fluorescein administration was performed, followed by endoscopic endonasal repair using an autologous fascial apposition graft and pedicled nasal-septal flap. Both the CSF leak and the pulmonary complications resolved following the operation with no symptoms at 11-month follow-up. This is the first reported case of spontaneous CSF rhinorrhea complicated by chronic aspiration and pneumonitis. Increased diagnostic complexity due to chronic pulmonary complications resulted in unnecessary interventions and treatment delays. Prompt recognition of spontaneous CSF leaks is essential to prevent potentially harmful complications.
Keywords: aspiration; cerebrospinal fluid; endonasal; endoscopic; pneumonitis.
Figures
References
-
- Wang E W Vandergrift W A III Schlosser R J Spontaneous CSF Leaks Otolaryngol Clin North Am 2011444845–856., vii - PubMed
-
- Yang Z, Wang B, Wang C, Liu P. Primary spontaneous cerebrospinal fluid rhinorrhea: a symptom of idiopathic intracranial hypertension? J Neurosurg. 2011;115(1):165–170. - PubMed
-
- Abuabara A. Cerebrospinal fluid rhinorrhoea: diagnosis and management. Med Oral Patol Oral Cir Bucal. 2007;12(5):E397–E400. - PubMed
-
- Motamedi M H, Sadidi A. Delayed cerebrospinal fluid leakage after head and facial trauma resulting in meningitis: a case report. J Oral Maxillofac Surg. 1998;56(3):365–367. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources