

Selective Insulin Resistance in the Kidney
- PMID: 27247938
- PMCID: PMC4876201
- DOI: 10.1155/2016/5825170
Selective Insulin Resistance in the Kidney
Abstract
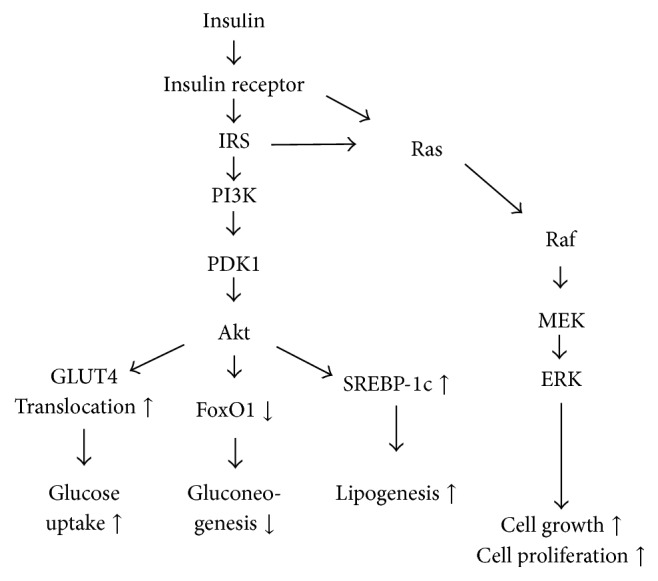
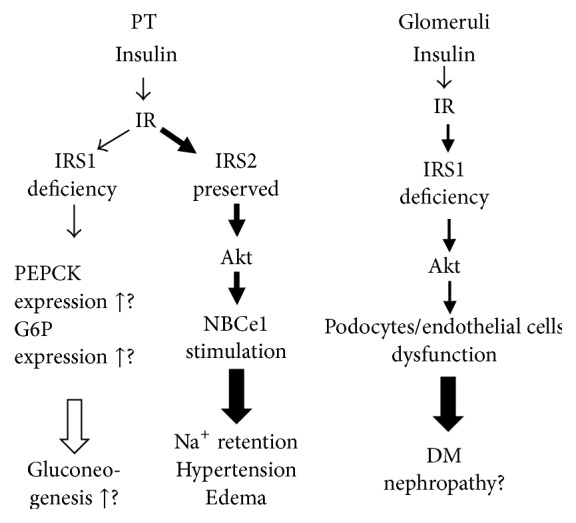
Insulin resistance has been characterized as attenuation of insulin sensitivity at target organs and tissues, such as muscle and fat tissues and the liver. The insulin signaling cascade is divided into major pathways such as the PI3K/Akt pathway and the MAPK/MEK pathway. In insulin resistance, however, these pathways are not equally impaired. For example, in the liver, inhibition of gluconeogenesis by the insulin receptor substrate (IRS) 2 pathway is impaired, while lipogenesis by the IRS1 pathway is preserved, thus causing hyperglycemia and hyperlipidemia. It has been recently suggested that selective impairment of insulin signaling cascades in insulin resistance also occurs in the kidney. In the renal proximal tubule, insulin signaling via IRS1 is inhibited, while insulin signaling via IRS2 is preserved. Insulin signaling via IRS2 continues to stimulate sodium reabsorption in the proximal tubule and causes sodium retention, edema, and hypertension. IRS1 signaling deficiency in the proximal tubule may impair IRS1-mediated inhibition of gluconeogenesis, which could induce hyperglycemia by preserving glucose production. In the glomerulus, the impairment of IRS1 signaling deteriorates the structure and function of podocyte and endothelial cells, possibly causing diabetic nephropathy. This paper mainly describes selective insulin resistance in the kidney, focusing on the proximal tubule.
Figures
References
-
- Hale L. J., Coward R. J. The insulin receptor and the kidney. Current Opinion in Nephrology and Hypertension. 2013;22:100–106. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
