

Practical Application of Columbia Classification for Focal Segmental Glomerulosclerosis
- PMID: 27247945
- PMCID: PMC4876206
- DOI: 10.1155/2016/9375753
Practical Application of Columbia Classification for Focal Segmental Glomerulosclerosis
Abstract
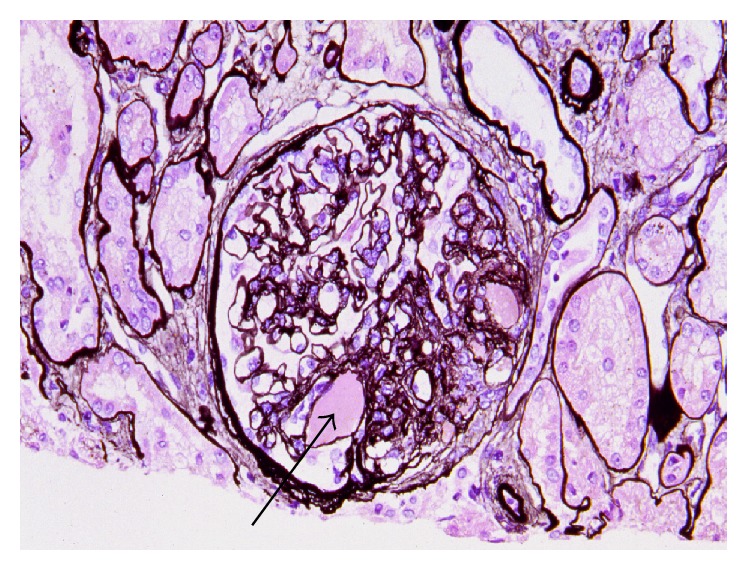
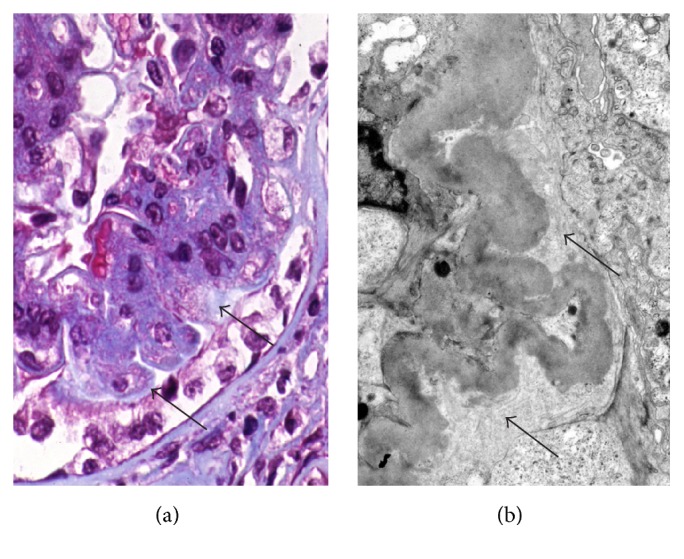
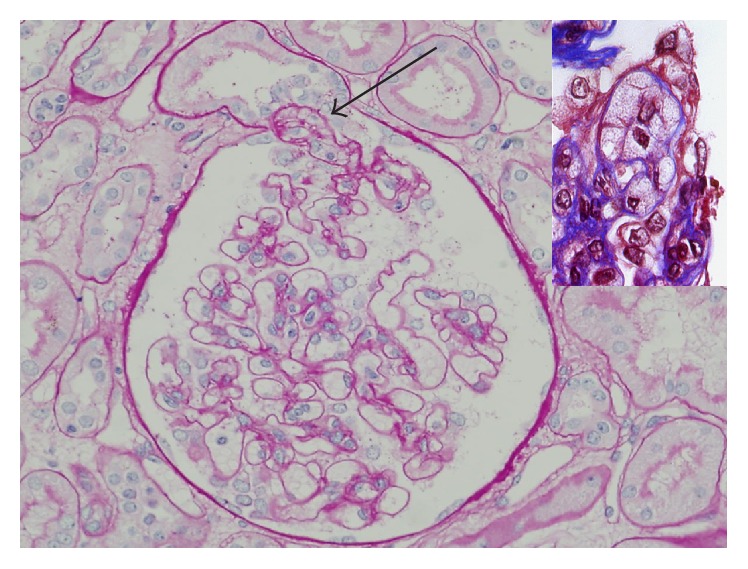
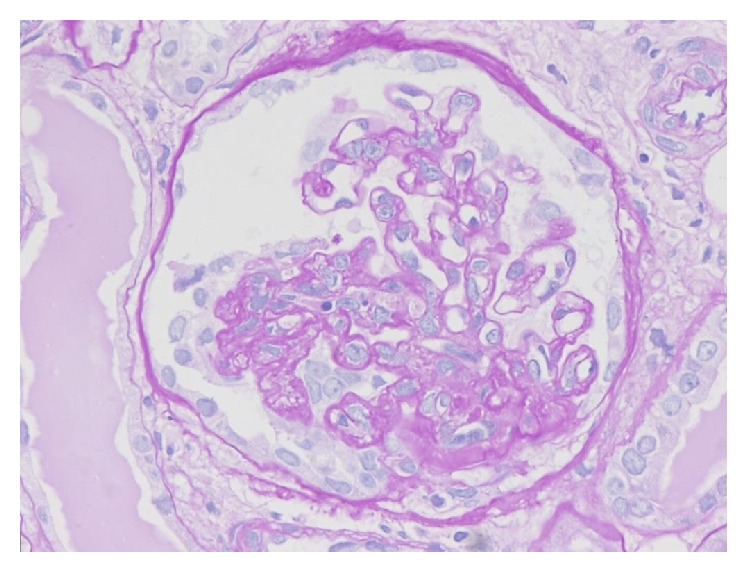
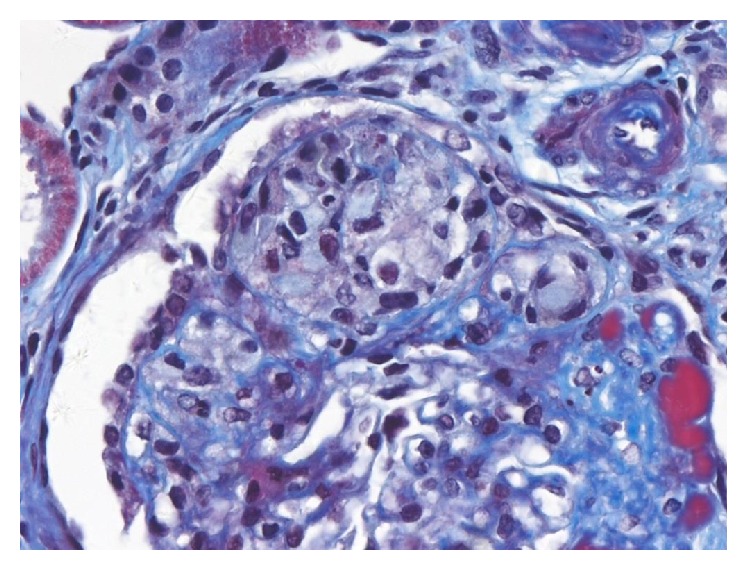
Focal segmental glomerulosclerosis (FSGS) is a heterogeneous clinicopathological entity. Two frameworks for the classification of FSGS have been described: etiologic and morphologic. The etiologic classification is distinguished among genetic, adaptive, virus-associated, drug-induced, and idiopathic types. Morphologic classification is commonly referred to as the Columbia classification published in 2004, which distinguishes five variants: collapsing, tip, cellular, perihilar, and not otherwise specified (NOS). This classification is based on light microscopic patterns with rigorously defined specific criteria, which can be applied to primary and secondary forms of FSGS, and has been widely used over the past 10 years both as a diagnostic and as a prognostic clinical tool. This paper defines common histopathological features of FSGS, distinguished characters among five variants, and points out the confusion about terminology of variants, because most were proposed in the past with different definitions. Despite good interobserver reproducibility of this classification system, difficulty in its application may arise in the interpretation of lesions with mixed features of more than one variant in the same tissue specimen and with late lesions, because other variants may evolve into the NOS variant over time.
Figures

References
-
- Jennette J. C., Olson J. L., Schwartz M. M., Silva F. G. Heptinstall's Pathology of the Kidney. 6th. Philadelphia, Pa, USA: Lippincott Williams & Wilkins; 2007.
-
- Kim Y. J. Pathology and classification of focal segmental glomerulosclerosis. Journal of the Korean Society of Pediatric Nephrology. 2012;16(1):21–31. doi: 10.3339/jkspn.2012.16.1.21. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
