

Subliminal gait initiation deficits in rapid eye movement sleep behavior disorder: A harbinger of freezing of gait?
- PMID: 27250871
- PMCID: PMC5115956
- DOI: 10.1002/mds.26665
Subliminal gait initiation deficits in rapid eye movement sleep behavior disorder: A harbinger of freezing of gait?
Abstract
Background: Muscle activity during rapid eye movement sleep is markedly increased in people with rapid eye movement sleep behavior disorder and people with Parkinson's disease (PD) who have freezing of gait. This study examined whether individuals with rapid eye movement sleep behavior disorder who do not have a diagnosis of PD show abnormalities in gait initiation that resemble the impairments observed in PD and whether there is a relationship between these deficits and the level of rapid eye movement sleep without atonia.
Methods: Gait initiation and polysomnography studies were conducted in 4 groups of 10 participants: rapid eye movement sleep behavior disorder, PD with and without freezing of gait, and controls.
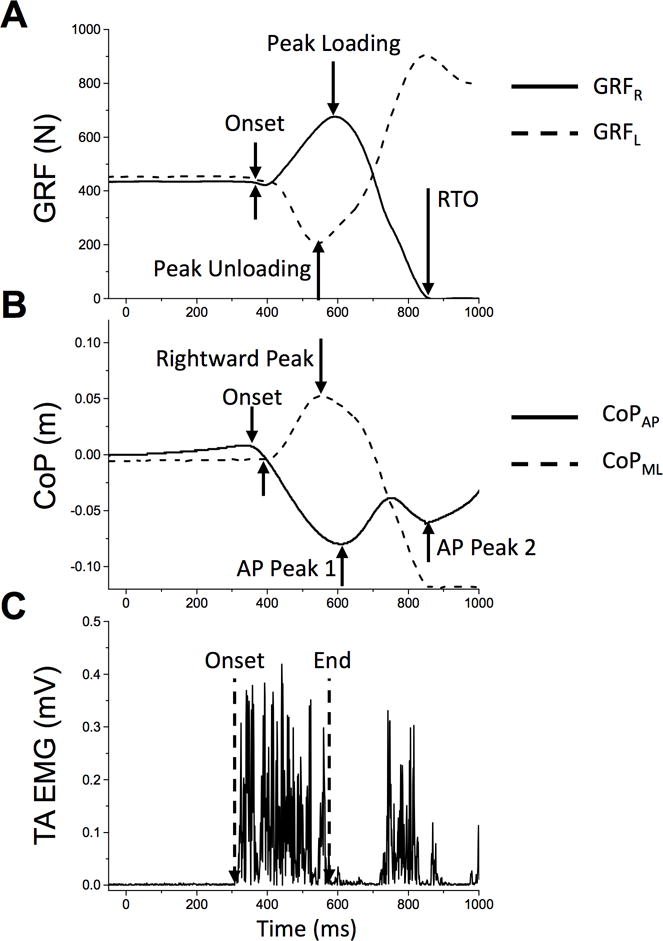
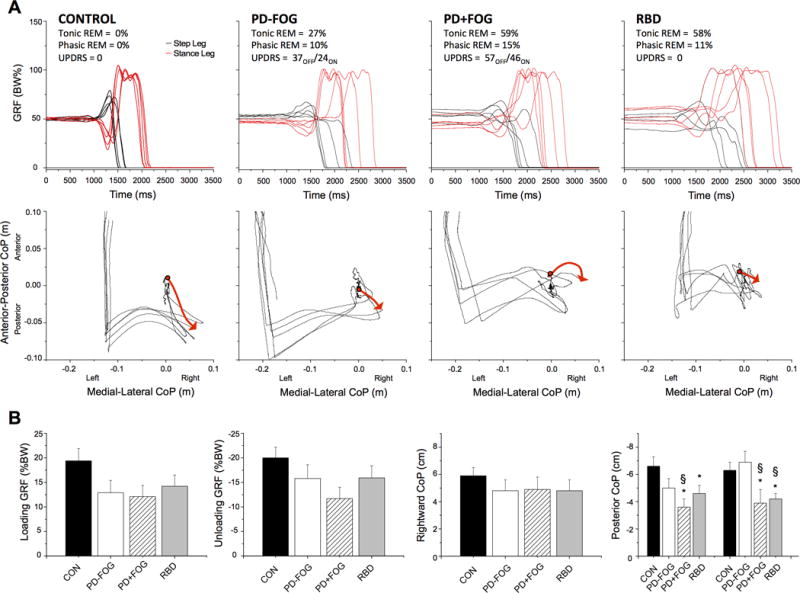
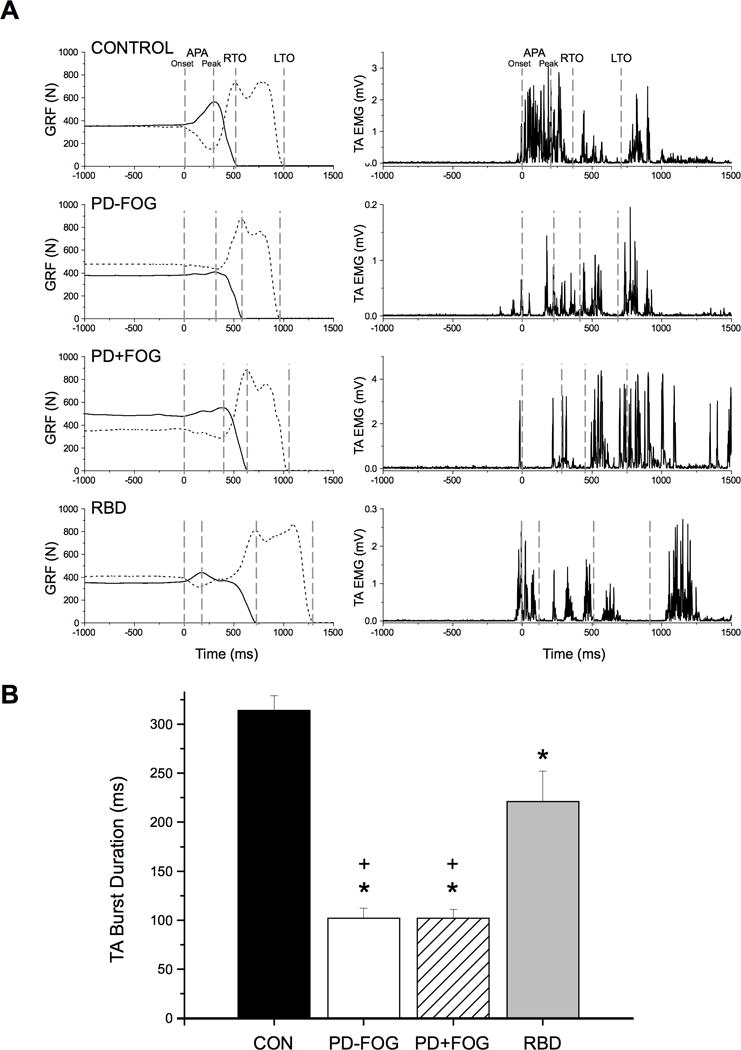
Results: Significant reductions were seen in the posterior shift of the center of pressure during the propulsive phase of gait initiation in the groups with rapid eye movement sleep behavior disorder and PD with freezing of gait when compared with controls and PD nonfreezers. These reductions negatively correlated with the amount of rapid eye movement sleep without atonia. The duration of the initial dorsiflexor muscle burst during gait initiation was significantly reduced in both PD groups and the rapid eye movement sleep behavior disorder cohort.
Conclusions: These results provide evidence that people with rapid eye movement sleep behavior disorder, prior to a diagnosis of a degenerative neurologic disorder, show alterations in the coupling of posture and gait similar to those seen in PD. The correlation between increased rapid eye movement sleep without atonia and deficits in forward propulsion during the push-off phase of gait initiation suggests that abnormities in the regulation of muscle tone during rapid eye movement sleep may be related to the pathogenesis of freezing of gait. © 2016 International Parkinson and Movement Disorder Society.
Keywords: PD; RBD; freezing; gait; sleep.
© 2016 International Parkinson and Movement Disorder Society.
Conflict of interest statement
Relevant Conflicts of Interest: Nothing to report.
Figures
References
-
- Schenck CH, Bundlie SR, Ettinger MG, Mahowald MW. Chronic behavioral disorders of human REM sleep: a new category of parasomnia. Sleep. 1986;9:293–308. - PubMed
-
- Boeve BF, Silber MH, Saper CB, et al. Pathophysiology of REM sleep behaviour disorder and relevance to neurodegenerative disease. Brain. 2007;130:2770–2788. - PubMed
-
- Schenck CH, Boeve BF, Mahowald MW. Delayed emergence of a parkinsonian disorder or dementia in 81% of older men initially diagnosed with idiopathic rapid eye movement sleep behavior disorder: a 16-year update on a previously reported series. Sleep Med. 2013;14:744–748. - PubMed
-
- Wetter TC, Trenkwalder C, Gershanik O, Hogl B. Polysomnographic measures in Parkinson’s disease: a comparison between patients with and without REM sleep disturbances. Wien Klin Wochenschr. 2001;113:249–253. - PubMed
-
- Gagnon JF, Bedard MA, Fantini ML, et al. REM sleep behavior disorder and REM sleep without atonia in Parkinson’s disease. Neurology. 2002;59:585–589. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
