

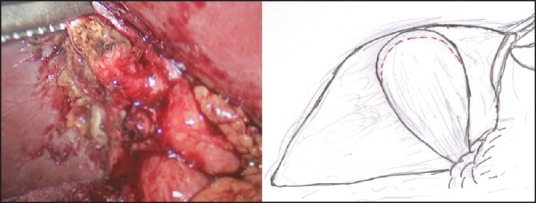
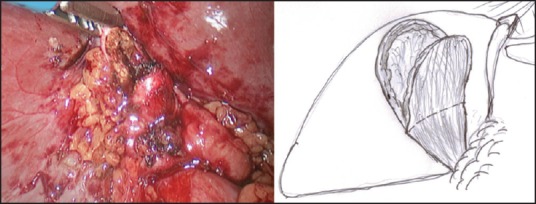
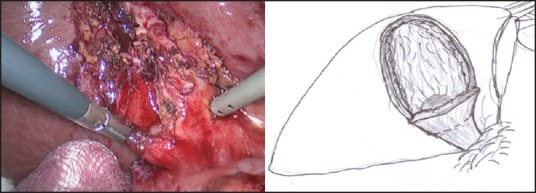
Laparoscopic modified subtotal cholecystectomy for difficult gall bladders: A single-centre experience
- PMID: 27251818
- PMCID: PMC5022512
- DOI: 10.4103/0972-9941.181323
Laparoscopic modified subtotal cholecystectomy for difficult gall bladders: A single-centre experience
Abstract
Aim: Laparoscopic cholecystectomy (LC) is considered the 'gold standard' intervention for gall bladder (GB) diseases. However, to avoid serious biliovascular injury, conversion is advocated for distorted anatomy at the Calot's triangle. The aim is to find out whether our technique of laparoscopic modified subtotal cholecystectomy (LMSC) is suitable, with an acceptable morbidity and outcome.
Patients and methods: A retrospective analysis of prospectively collected data of 993 consecutive patients who underwent cholecystectomy was done at a large District General Hospital (DGH) between August 2007 and January 2015. The data are as follows: Patient's demographics, operative details including intra- and postoperative complications, postoperative stay including follow-up that was recorded and analysed.
Results: A total of 993 patients (263 males and 730 female) were included. The median age was 52*(18-89) years. Out of the 993 patients, 979 (98.5%) and 14 (1.5%) were listed for laparoscopic and open cholecystectomy, respectively. Of the 979 patients, 902 (92%) and 64 (6.5%) patients underwent LC ± on-table cholangiography (OTC) and LMSC ± OTC, respectively, with a median stay of 1* (0-15) days. Of the 64 patients, 55 (86%) had dense adhesions, 22 (34%) had acute inflammation, 19 (30%) had severe contraction, 12 (19%) had empyema, 7 (11%) had Mirizzi's syndrome and 2 (3%) had gangrenous GB. The mean operative time was 120 × (50-180) min [Table 1]. Six (12%) patients required endoscopic retrograde cholangiopancreatography (ERCP) postoperatively, and there were four (6%) readmissions in a follow-up of 30 × (8-76) months. The remaining 13 (1.3%) patients underwent laparoscopic cholecystectomy converted to an open cholecystectomy. The median stay for open/laparoscopic cholecystectomy converted to open cholecystectomy was 5 × (1-12) days.
Conclusion: Our technique of LMSC avoided conversion in 6.5% patients and believe that it is feasible and safe for difficult GBs with a positive outcome.
Figures

References
-
- Begos DG, Modlin IM. Laparoscopic cholecystectomy: From gimmick to gold standard. J Clin Gastroenterol. 1994;19:325–30. - PubMed
-
- Gurusamy KS, Davidson C, Gluud C, Davidson BR. Early versus delayed laparoscopic cholecystectomy for people with acute cholecystitis. Cochrane Database Syst Rev. 2013;6:CD005440. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources