

A new saccadic indicator of peripheral vestibular function based on the video head impulse test
- PMID: 27251884
- PMCID: PMC4977115
- DOI: 10.1212/WNL.0000000000002827
A new saccadic indicator of peripheral vestibular function based on the video head impulse test
Abstract
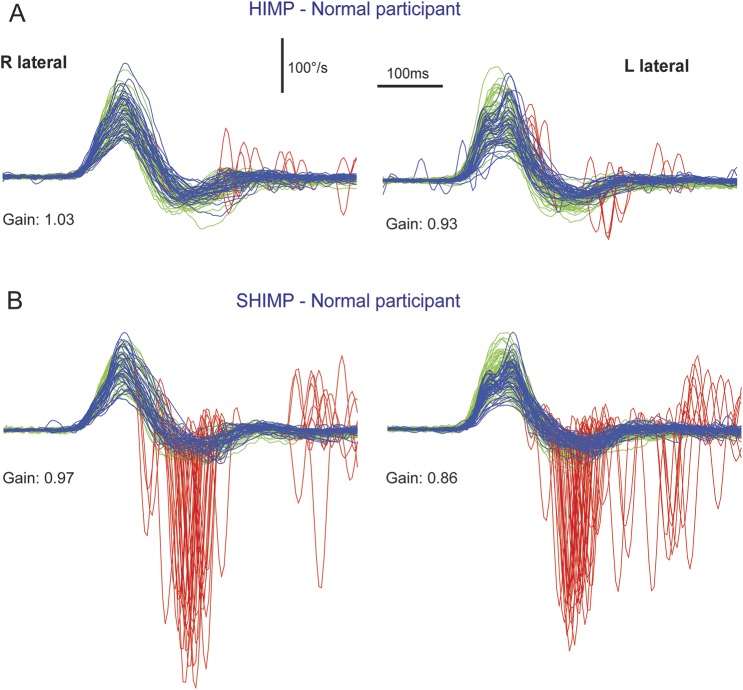
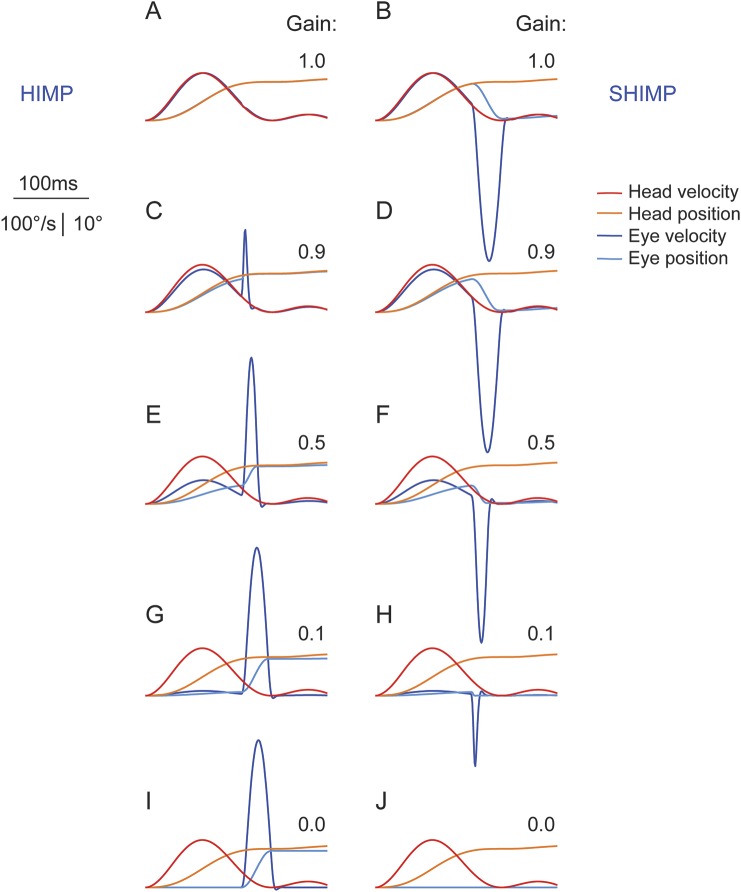
Objective: While compensatory saccades indicate vestibular loss in the conventional head impulse test paradigm (HIMP), in which the participant fixates an earth-fixed target, we investigated a complementary suppression head impulse paradigm (SHIMP), in which the participant is fixating a head-fixed target to elicit anticompensatory saccades as a sign of vestibular function.
Methods: HIMP and SHIMP eye movement responses were measured with the horizontal video head impulse test in patients with unilateral vestibular loss, patients with bilateral vestibular loss, and in healthy controls.
Results: Vestibulo-ocular reflex gains showed close correlation (R(2) = 0.97) with slightly lower SHIMP than HIMP gains (mean gain difference 0.06 ± 0.05 SD, p < 0.001). However, the 2 paradigms produced complementary catch-up saccade patterns: HIMP elicited compensatory saccades in patients but rarely in controls, whereas SHIMP elicited large anticompensatory saccades in controls, but smaller or no saccades in bilateral vestibular loss. Unilateral vestibular loss produced covert saccades in HIMP, but later and smaller saccades in SHIMP toward the affected side. Cumulative HIMP and SHIMP saccade amplitude differentiated patients from controls with high sensitivity and specificity.
Conclusions: While compensatory saccades indicate vestibular loss in conventional HIMP, anticompensatory saccades in SHIMP using a head-fixed target indicate vestibular function. SHIMP saccades usually appear later than HIMP saccades, therefore being more salient to the naked eye and facilitating vestibulo-ocular reflex gain measurements. The new paradigm is intuitive and easy to explain to patients, and the SHIMP results complement those from the standard video head impulse test.
Classification of evidence: This case-control study provides Class III evidence that SHIMP accurately identifies patients with unilateral or bilateral vestibulopathies.
© 2016 American Academy of Neurology.
Figures



References
-
- Halmagyi GM, Curthoys IS. A clinical sign of canal paresis. Arch Neurol 1988;45:737–739. - PubMed
-
- Weber KP, Aw ST, Todd MJ, McGarvie LA, Curthoys IS, Halmagyi GM. Head impulse test in unilateral vestibular loss: vestibulo-ocular reflex and catch-up saccades. Neurology 2008;70:454–463. - PubMed
-
- Barin K. Interpretation and usefulness of caloric testing. In: Jacobson GP, Shepard NT, editors. Balance Function Assessment and Management, 2nd ed. San Diego: Plural Publishing; 2016:319–345.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials