

A Longitudinal Follow-up of Autoimmune Polyendocrine Syndrome Type 1
- PMID: 27253668
- PMCID: PMC4971337
- DOI: 10.1210/jc.2016-1821
A Longitudinal Follow-up of Autoimmune Polyendocrine Syndrome Type 1
Abstract
Context: Autoimmune polyendocrine syndrome type 1 (APS1) is a childhood-onset monogenic disease defined by the presence of two of the three major components: hypoparathyroidism, primary adrenocortical insufficiency, and chronic mucocutaneous candidiasis (CMC). Information on longitudinal follow-up of APS1 is sparse.
Objective: To describe the phenotypes of APS1 and correlate the clinical features with autoantibody profiles and autoimmune regulator (AIRE) mutations during extended follow-up (1996-2016).
Patients: All known Norwegian patients with APS1.
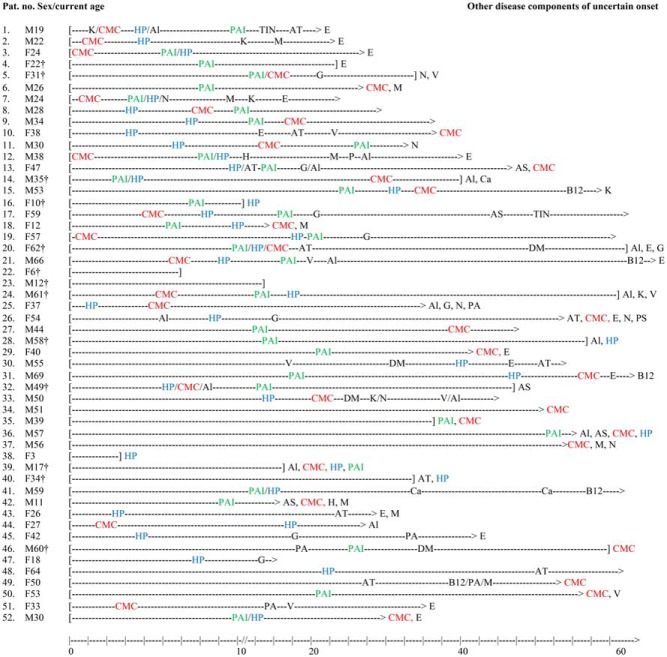
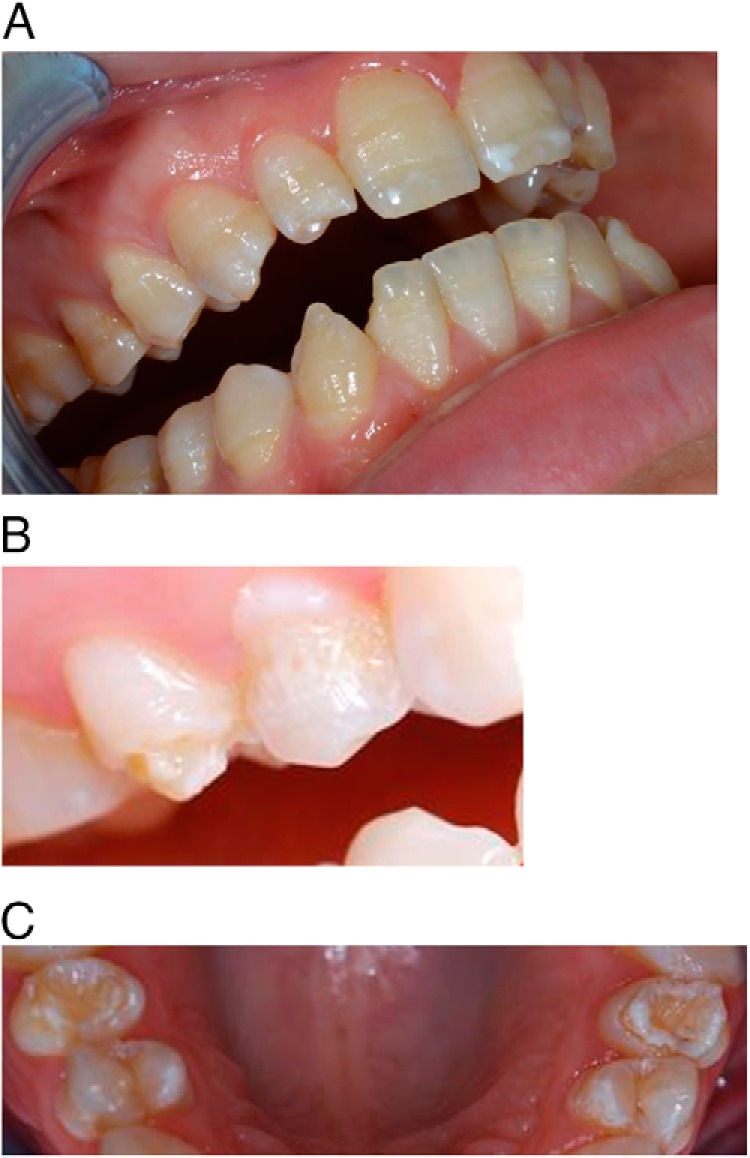
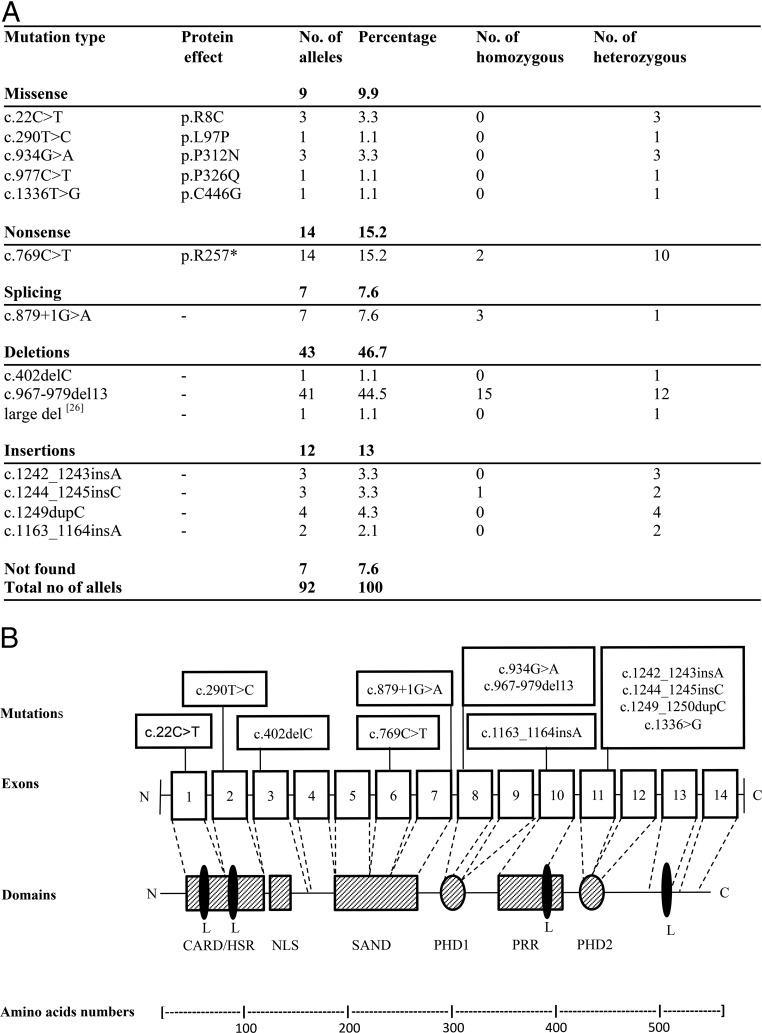
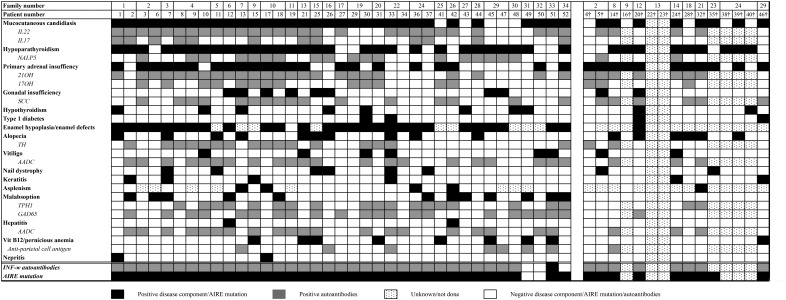
Results: Fifty-two patients from 34 families were identified. The majority presented with one of the major disease components during childhood. Enamel hypoplasia, hypoparathyroidism, and CMC were the most frequent components. With age, most patients presented three to five disease manifestations, although some had milder phenotypes diagnosed in adulthood. Fifteen of the patients died during follow-up (median age at death, 34 years) or were deceased siblings with a high probability of undisclosed APS1. All except three had interferon-ω) autoantibodies, and all had organ-specific autoantibodies. The most common AIRE mutation was c.967_979del13, found in homozygosity in 15 patients. A mild phenotype was associated with the splice mutation c.879+1G>A. Primary adrenocortical insufficiency and type 1 diabetes were associated with protective human leucocyte antigen genotypes.
Conclusions: Multiple presumable autoimmune manifestations, in particular hypoparathyroidism, CMC, and enamel hypoplasia, should prompt further diagnostic workup using autoantibody analyses (eg, interferon-ω) and AIRE sequencing to reveal APS1, even in adults. Treatment is complicated, and mortality is high. Structured follow-up should be performed in a specialized center.
Figures
References
-
- Ahonen P, Myllärniemi S, Sipilä I, Perheentupa J. Clinical variation of autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy (APECED) in a series of 68 patients. N Engl J Med. 1990;322:1829–1836. - PubMed
-
- Husebye ES, Perheentupa J, Rautemaa R, Kämpe O. Clinical manifestations and management of patients with autoimmune polyendocrine syndrome type I. J Intern Med. 2009;265:514–529. - PubMed
-
- Wolff AS, Erichsen MM, Meager A, et al. Autoimmune polyendocrine syndrome type 1 in Norway: phenotypic variation, autoantibodies, and novel mutations in the autoimmune regulator gene. J Clin Endocrinol Metab. 2007;92:595–603. - PubMed
-
- Bensing S, Brandt L, Tabaroj F, et al. Increased death risk and altered cancer incidence pattern in patients with isolated or combined autoimmune primary adrenocortical insufficiency. Clin Endocrinol (Oxf). 2008;69:697–704. - PubMed
-
- Nagamine K, Peterson P, Scott HS, et al. Positional cloning of the APECED gene. Nat Genet. 1997;17:393–398. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
