

Prediction of infarction development after endovascular stroke therapy with dual-energy computed tomography
- PMID: 27255400
- PMCID: PMC5591619
- DOI: 10.1007/s00330-016-4412-5
Prediction of infarction development after endovascular stroke therapy with dual-energy computed tomography
Abstract
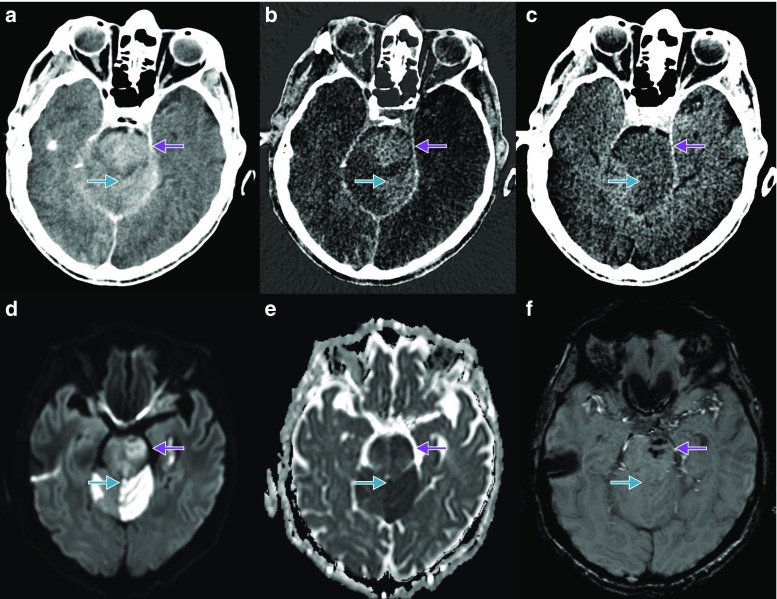
Objectives: After intraarterial recanalisation (IAR), the haemorrhage and the blood-brain barrier (BBB) disruption can be distinguished using dual-energy computed tomography (DECT). The aim of the present study was to investigate whether future infarction development can be predicted from DECT.
Methods: DECT scans of 20 patients showing 45 BBB disrupted areas after IAR were assessed and compared with follow-up examinations. Receiver operator characteristic (ROC) analyses using densities from the iodine map (IM) and virtual non-contrast (VNC) were performed.
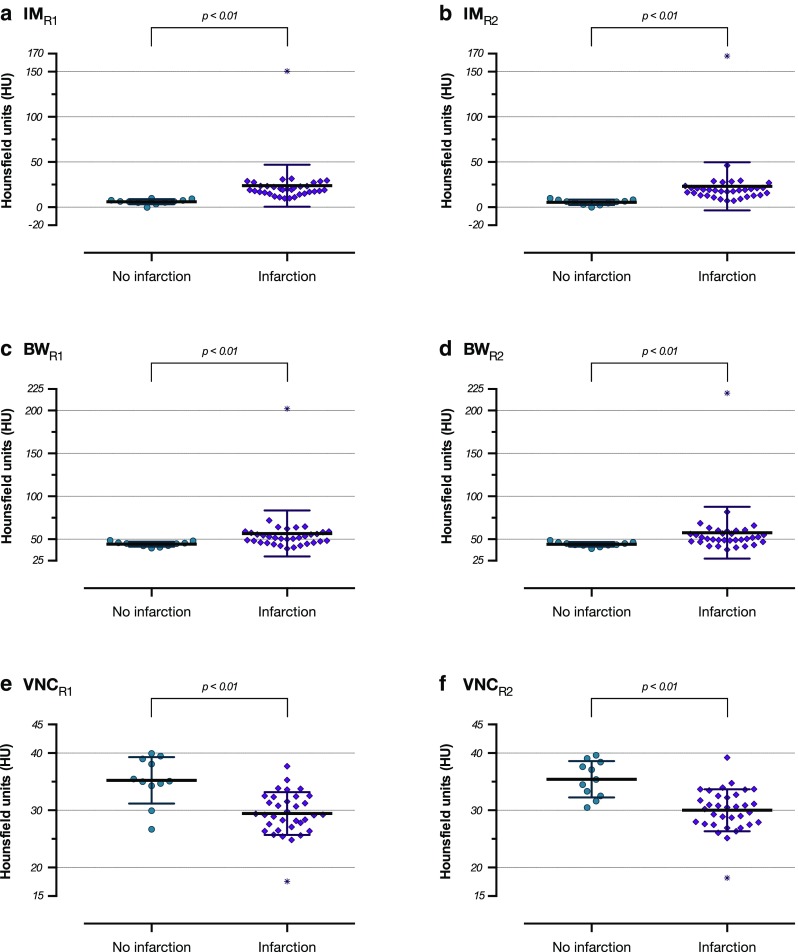
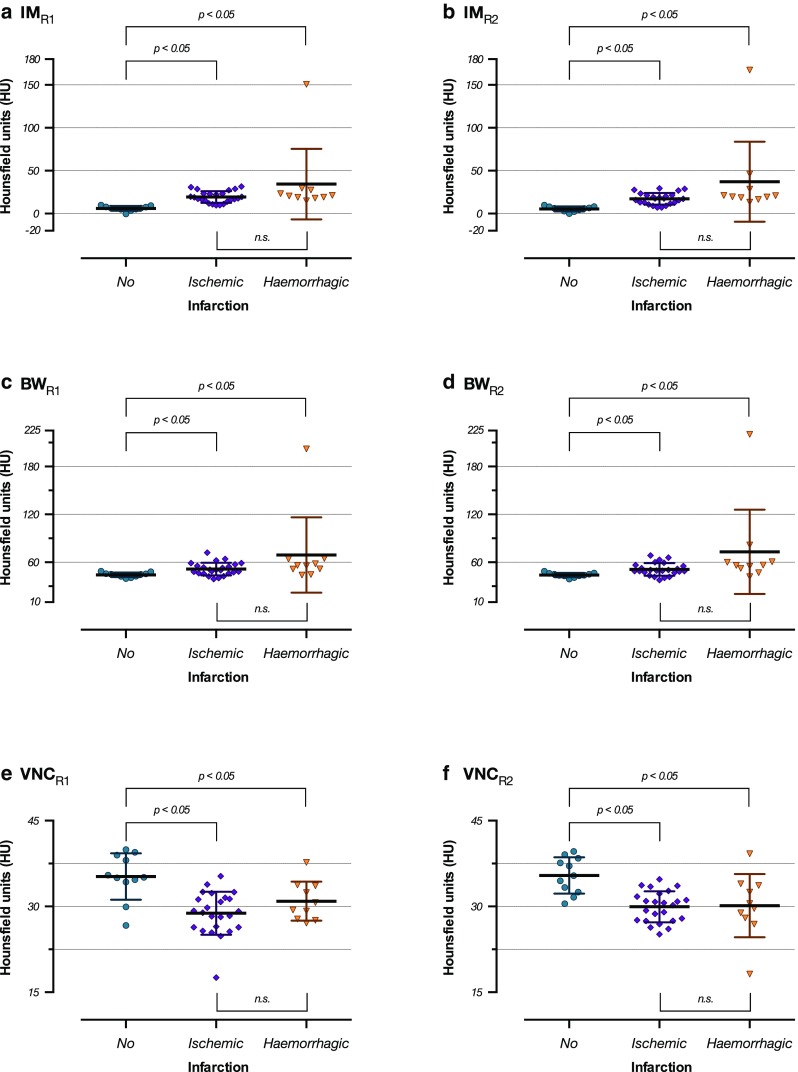
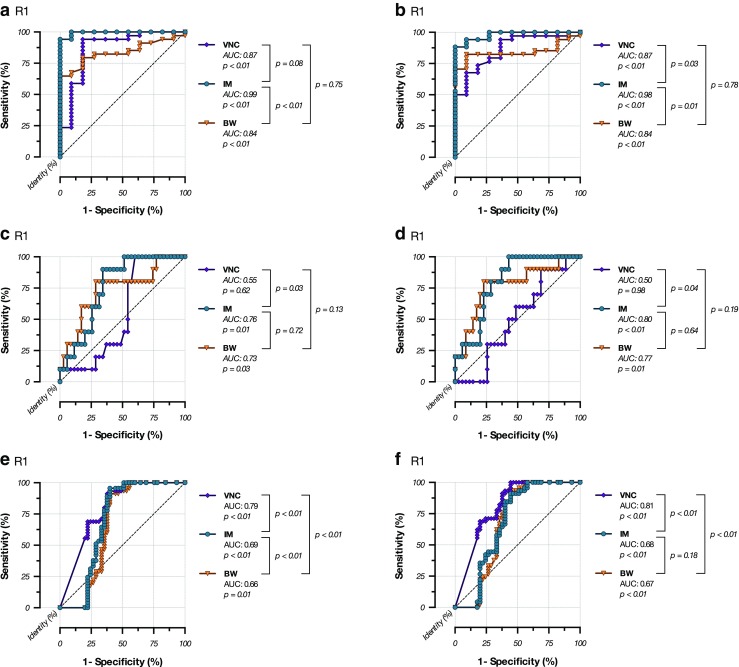
Results: Future infarction areas are denser than future non-infarction areas on IM series (23.44 ± 24.86 vs. 5.77 ± 2.77; p < 0.0001) and more hypodense on VNC series (29.71 ± 3.33 vs. 35.33 ± 3.50; p < 0.0001). ROC analyses for the IM series showed an area under the curve (AUC) of 0.99 (cut-off: <9.97 HU; p < 0.05; sensitivity 91.18 %; specificity 100.00 %; accuracy 0.93) for the prediction of future infarctions. The AUC for the prediction of haemorrhagic infarctions was 0.78 (cut-off >17.13 HU; p < 0.05; sensitivity 90.00 %; specificity 62.86 %; accuracy 0.69). The VNC series allowed prediction of infarction volume.
Conclusions: Future infarction development after IAR can be reliably predicted with the IM series. The prediction of haemorrhages and of infarction size is less reliable.
Key points: • The IM series (DECT) can predict future infarction development after IAR. • Later haemorrhages can be predicted using the IM and the BW series. • The volume of definable hypodense areas in VNC correlates with infarction volume.
Keywords: Blood-brain barrier disruption; Cerebral infarction; Dual-energy computed tomography; Endovascular stroke therapy; Intracranial haemorrhage.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
