

Explaining outcomes in major system change: a qualitative study of implementing centralised acute stroke services in two large metropolitan regions in England
- PMID: 27255558
- PMCID: PMC4891887
- DOI: 10.1186/s13012-016-0445-z
Explaining outcomes in major system change: a qualitative study of implementing centralised acute stroke services in two large metropolitan regions in England
Abstract
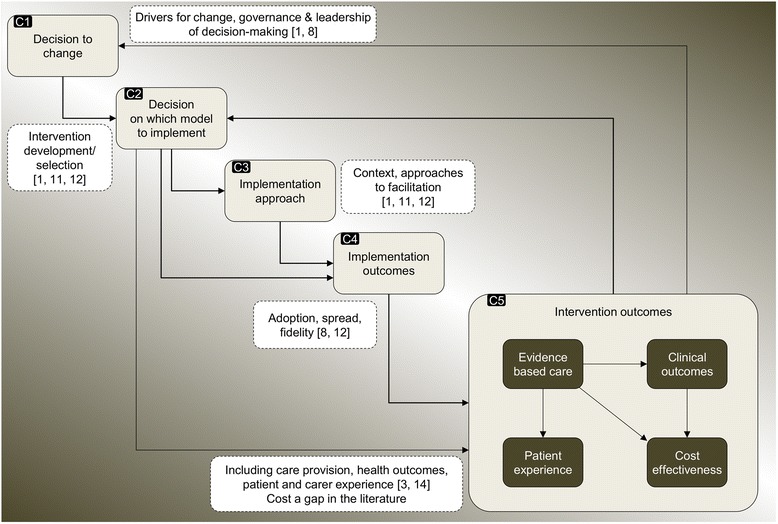
Background: Implementing major system change in healthcare is not well understood. This gap may be addressed by analysing change in terms of interrelated components identified in the implementation literature, including decision to change, intervention selection, implementation approaches, implementation outcomes, and intervention outcomes.
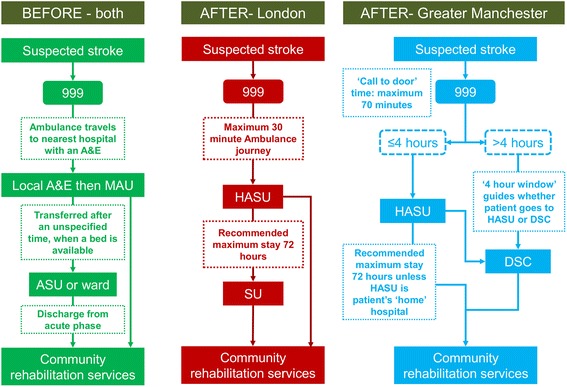
Methods: We conducted a qualitative study of two cases of major system change: the centralisation of acute stroke services in Manchester and London, which were associated with significantly different implementation outcomes (fidelity to referral pathway) and intervention outcomes (provision of evidence-based care, patient mortality). We interviewed stakeholders at national, pan-regional, and service-levels (n = 125) and analysed 653 documents. Using a framework developed for this study from the implementation science literature, we examined factors influencing implementation approaches; how these approaches interacted with the models selected to influence implementation outcomes; and their relationship to intervention outcomes.
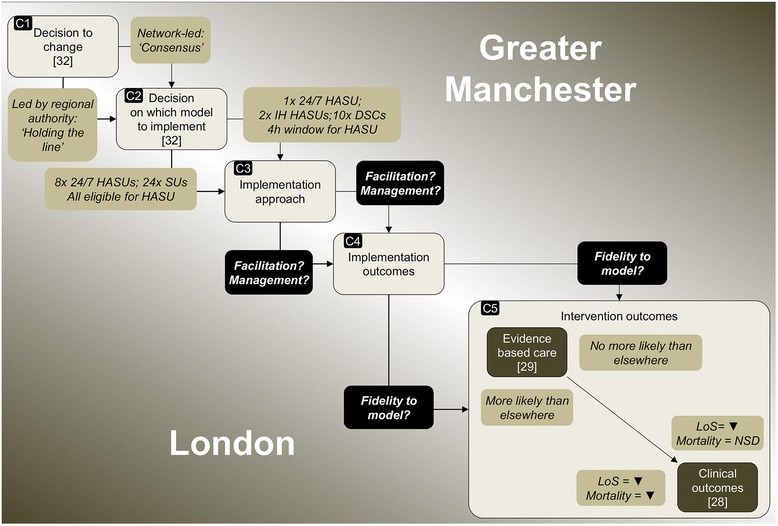
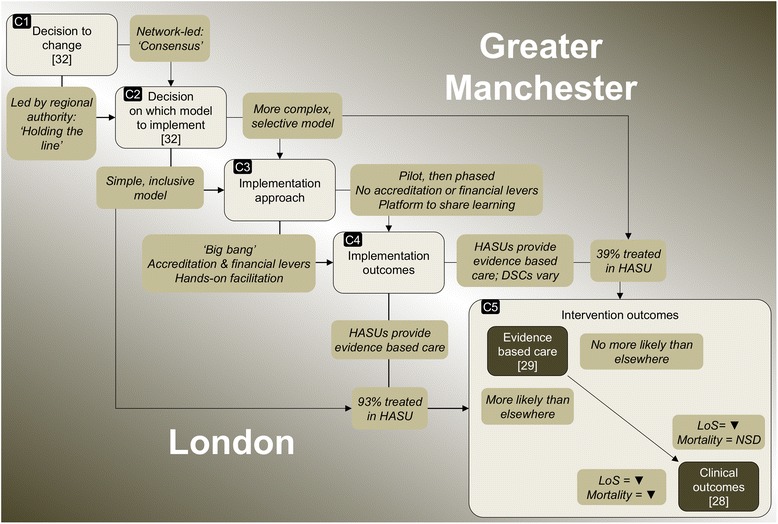
Results: London and Manchester's differing implementation outcomes were influenced by the different service models selected and implementation approaches used. Fidelity to the referral pathway was higher in London, where a 'simpler', more inclusive model was used, implemented with a 'big bang' launch and 'hands-on' facilitation by stroke clinical networks. In contrast, a phased approach of a more complex pathway was used in Manchester, and the network acted more as a platform to share learning. Service development occurred more uniformly in London, where service specifications were linked to financial incentives, and achieving standards was a condition of service launch, in contrast to Manchester. 'Hands-on' network facilitation, in the form of dedicated project management support, contributed to achievement of these standards in London; such facilitation processes were less evident in Manchester.
Conclusions: Using acute stroke service centralisation in London and Manchester as an example, interaction between model selected and implementation approaches significantly influenced fidelity to the model. The contrasting implementation outcomes may have affected differences in provision of evidence-based care and patient mortality. The framework used in this analysis may support planning and evaluating major system changes, but would benefit from application in different healthcare contexts.
Keywords: Centralisation of healthcare; Evaluation; Implementation approaches; Implementation outcomes; Stroke care.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
