

How Regrouping Alerts in Computerized Physician Order Entry Layout Influences Physicians' Prescription Behavior: Results of a Crossover Randomized Trial
- PMID: 27255612
- PMCID: PMC4911510
- DOI: 10.2196/humanfactors.5320
How Regrouping Alerts in Computerized Physician Order Entry Layout Influences Physicians' Prescription Behavior: Results of a Crossover Randomized Trial
Abstract
Background: As demonstrated in several publications, low positive predictive value alerts in computerized physician order entry (CPOE) induce fatigue and may interrupt physicians unnecessarily during prescription of medication. Although it is difficult to increase the consideration of medical alerts by physician through an improvement of their predictive value, another approach consists to act on the way they are presented. The interruption management model inspired us to propose an alternative alert display strategy of regrouping the alerts in the screen layout, as a possible solution for reducing the interruption in physicians' workflow.
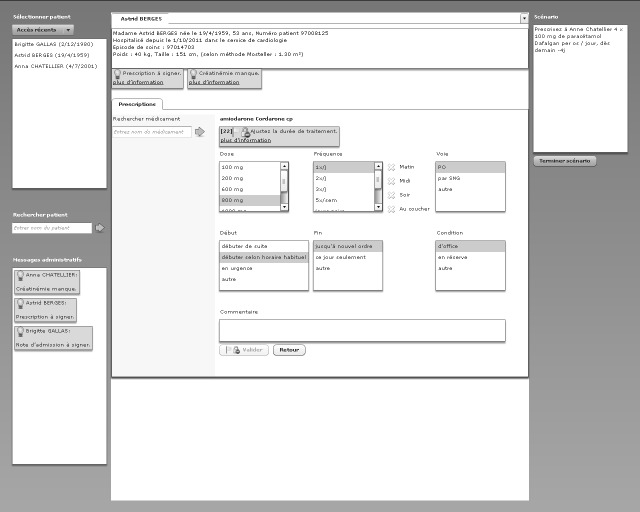
Objective: In this study, we compared 2 CPOE designs based on a particular alert presentation strategy: one design involved regrouping the alerts in a single place on the screen, and in the other, the alerts were located next to the triggering information. Our objective was to evaluate experimentally whether the new design led to fewer interruptions in workflow and if it affected alert handling.
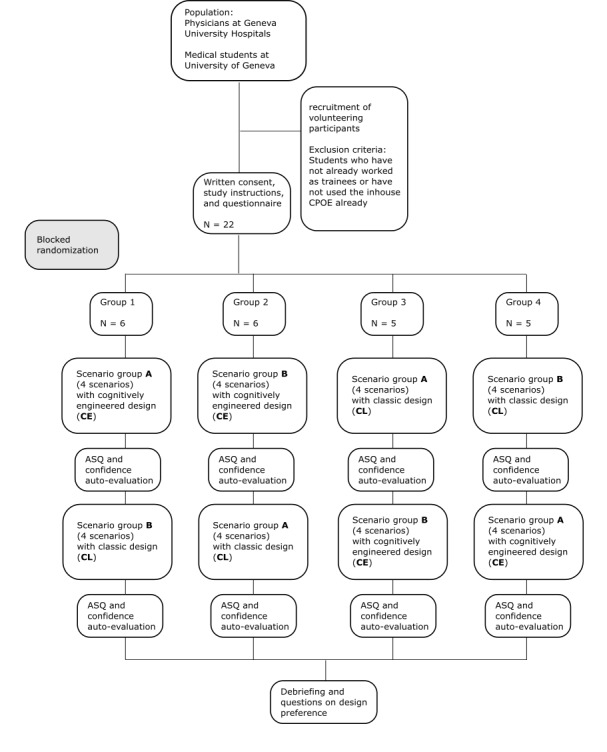
Methods: The 2 CPOE designs were compared in a controlled crossover randomized trial. All interactions with the system and eye movements were stored for quantitative analysis.
Results: The study involved a group of 22 users consisting of physicians and medical students who solved medical scenarios containing prescription tasks. Scenario completion time was shorter when the alerts were regrouped (mean 117.29 seconds, SD 36.68) than when disseminated on the screen (mean 145.58 seconds, SD 75.07; P=.045). Eye tracking revealed that physicians fixated longer on alerts in the classic design (mean 119.71 seconds, SD 76.77) than in the centralized alert design (mean 70.58 seconds, SD 33.53; P=.001). Visual switches between prescription and alert areas, indicating interruption, were reduced with centralized alerts (mean 41.29, SD 21.26) compared with the classic design (mean 57.81, SD 35.97; P=.04). Prescription behavior (ie, prescription changes after alerting), however, did not change significantly between the 2 strategies of display. The After-Scenario Questionnaire (ASQ) that was filled out after each scenario showed that overall satisfaction was significantly rated lower when alerts were regrouped (mean 4.37, SD 1.23) than when displayed next to the triggering information (mean 5.32, SD 0.94; P=.02).
Conclusions: Centralization of alerts in a table might be a way to motivate physicians to manage alerts more actively, in a meaningful way, rather than just being interrupted by them. Our study could not provide clear recommendations yet, but provides objective data through a cognitive psychological approach. Future tests should work on standardized scenarios that would enable to not only measure physicians' behavior (visual fixations and handling of alerts) but also validate those actions using clinical criteria.
Keywords: User-Computer Interface; adverse drug reaction reporting systems; clinical decision support systems; eye tracking; medical order entry systems.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures

References
-
- Kuperman GJ, Bobb A, Payne TH, Avery AJ, Gandhi TK, Burns G, Classen DC, Bates DW. Medication-related clinical decision support in computerized provider order entry systems: a review. J Am Med Inform Assoc. 2007;14(1):29–40. doi: 10.1197/jamia.M2170. http://jamia.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=17068355 - DOI - PMC - PubMed
-
- Schedlbauer A, Prasad V, Mulvaney C, Phansalkar S, Stanton W, Bates DW, Avery AJ. What evidence supports the use of computerized alerts and prompts to improve clinicians' prescribing behavior? J Am Med Inform Assoc. 2009;16(4):531–8. doi: 10.1197/jamia.M2910. http://jamia.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=19390110 - DOI - PMC - PubMed
-
- Garg AX, Adhikari Neill K J. McDonald H, Rosas-Arellano MP, Devereaux PJ, Beyene J, Sam J, Haynes RB. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review. JAMA. 2005 Mar 9;293(10):1223–38. doi: 10.1001/jama.293.10.1223. - DOI - PubMed
-
- van der Sijs H, Aarts J, Vulto A, Berg M. Overriding of drug safety alerts in computerized physician order entry. J Am Med Inform Assoc. 2006;13(2):138–47. doi: 10.1197/jamia.M1809. http://jamia.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=16357358 - DOI - PMC - PubMed
-
- Sittig DF, Wright A, Osheroff JA, Middleton B, Teich JM, Ash JS, Campbell E, Bates DW. Grand challenges in clinical decision support. J Biomed Inform. 2008 Apr;41(2):387–92. doi: 10.1016/j.jbi.2007.09.003. http://linkinghub.elsevier.com/retrieve/pii/S1532-0464(07)00104-9 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
