

Uveitic macular edema
- PMID: 27256304
- PMCID: PMC5129852
- DOI: 10.1038/eye.2016.115
Uveitic macular edema
Abstract
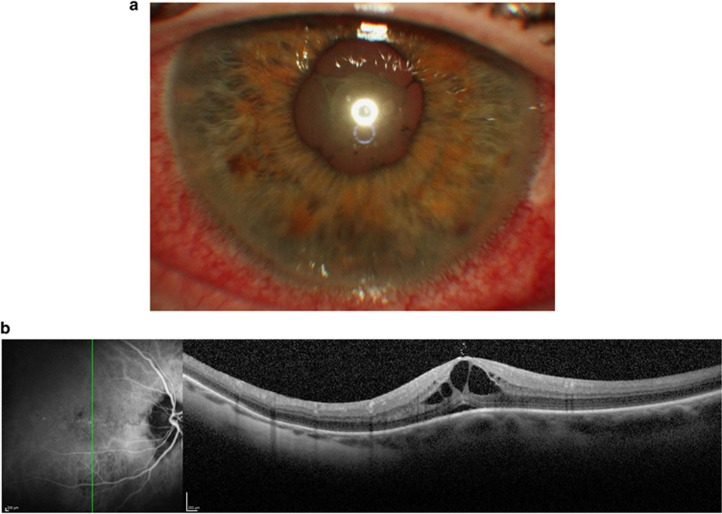
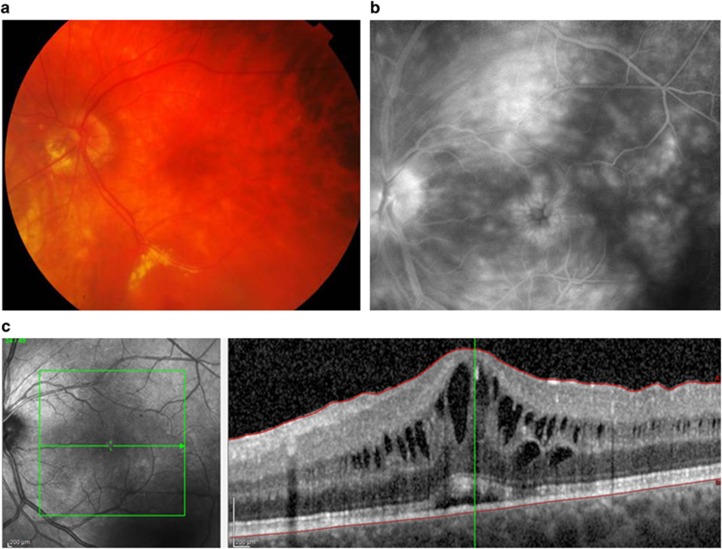
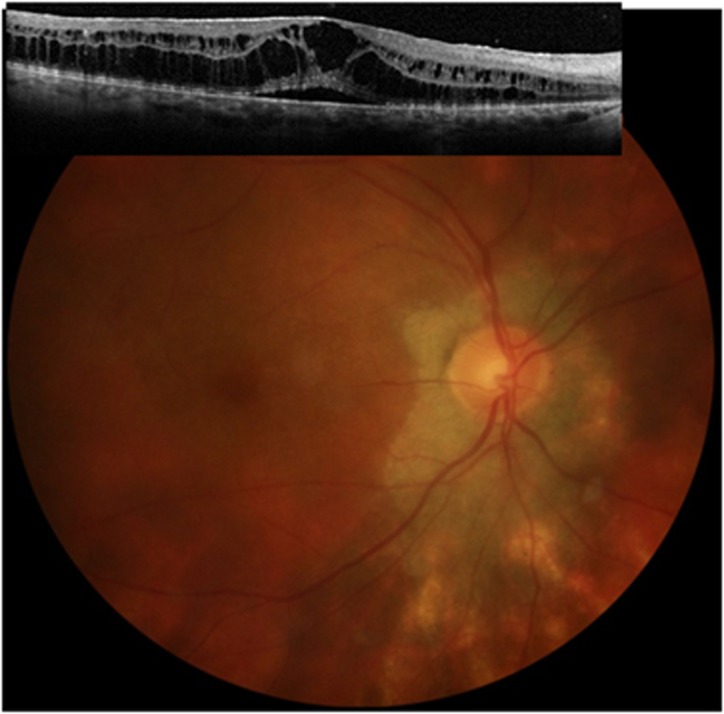
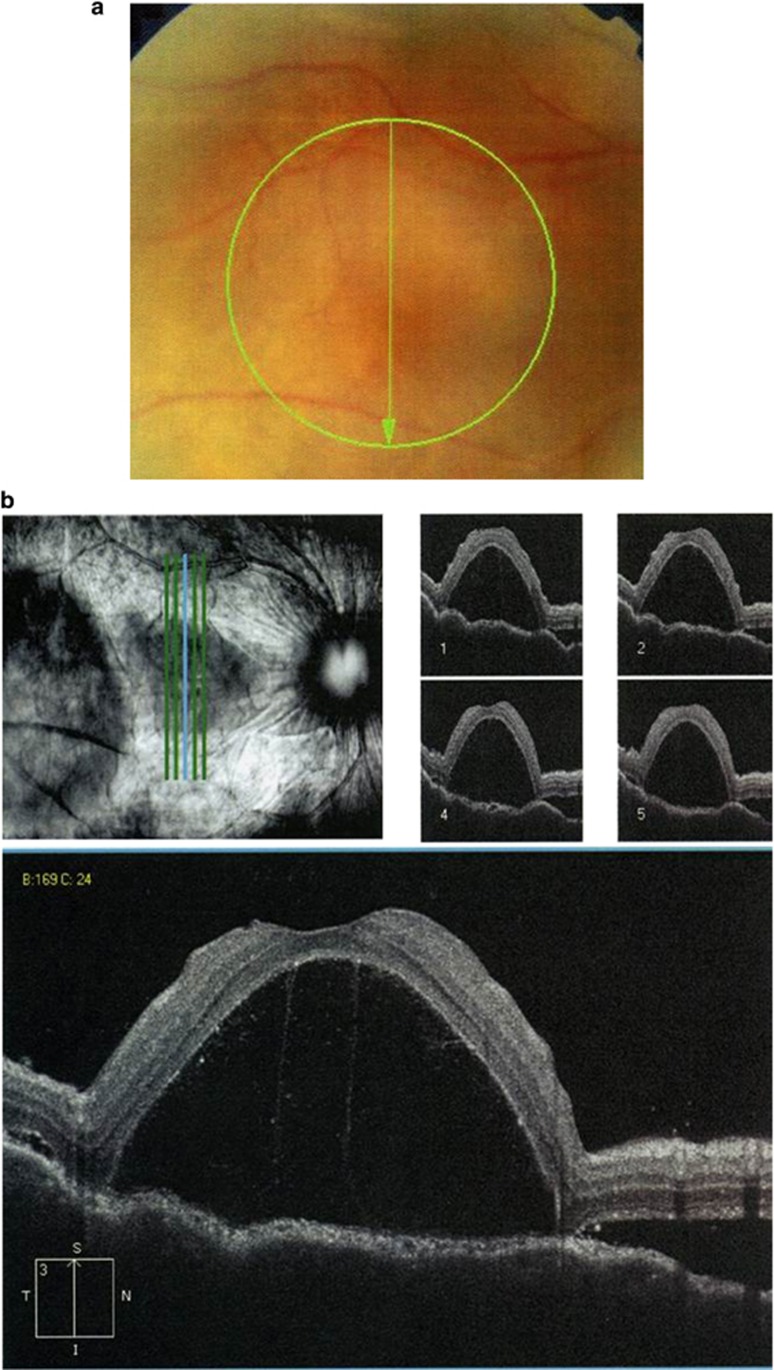
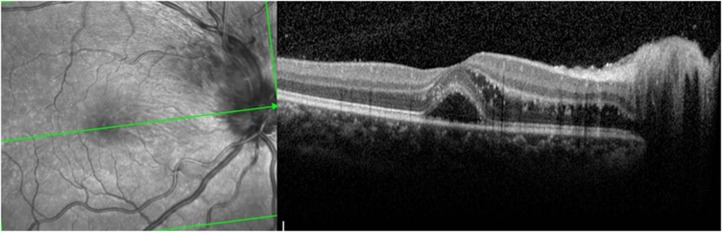
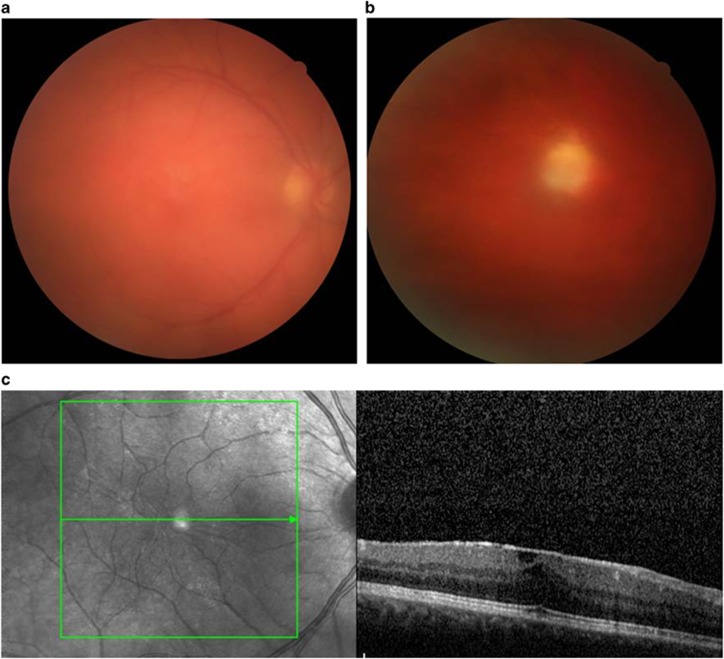
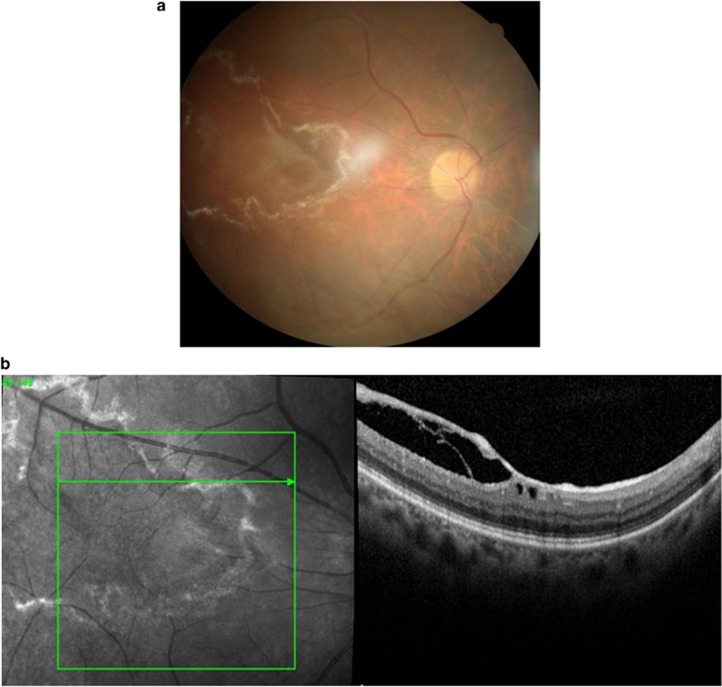
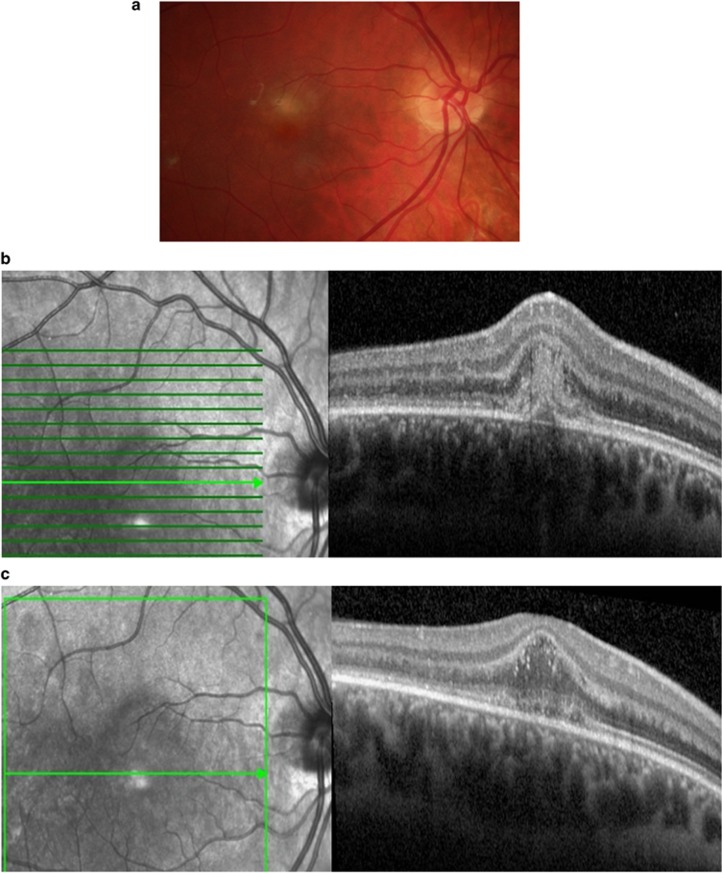
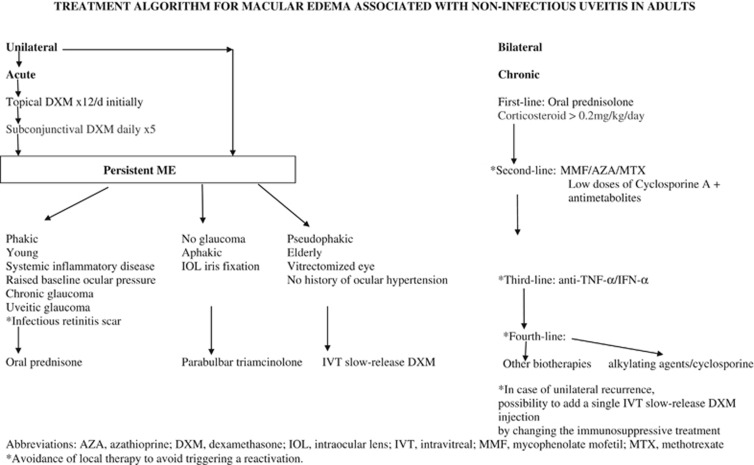
Macular edema (ME) may complicate anterior, intermediate, and posterior uveitis, which may be because of various infectious, neoplastic or autoimmune etiologies. BRB breakdown is involved in the pathogenesis of Uveitic ME (UME). Optical coherence tomography has become a standard tool to confirm the diagnosis of macular thickening, due to its non-invasive, reproducible, and sensitive features. Retinal fluorescein and indocyanine green angiography is helpful to study the macula and screen for associated vasculitis, detect ischemic areas and preretinal, prepapillary or choroidal neovascular complications, and it may provide information about the etiology and be needed to assess the therapeutic response. UME due to an infection or neoplastic infiltration may require a specific treatment. If it remains persistent or occurs in other etiologies, immunomodulatory treatments may be needed. Intravitreal, subconjunctival, or subtenon corticosteroids are widely used. Their local use is contraindicated in glaucoma patients and limited by their short-lasting action. In case of bilateral sight-threatening chronic posterior uveitis, systemic treatments are usually needed, and corticosteroids are used as the standard first-line therapy. In order to reduce the daily steroid dose, immunosuppressive or immunomodulatory agents may be added, some of them being now available intravitreally. Ongoing prospective studies are assessing biotherapies and immunomodulators to determine their safety and efficacy in this indication.
Figures
Similar articles
-
[Uveitic macular edema].J Fr Ophtalmol. 2015 Jan;38(1):74-81. doi: 10.1016/j.jfo.2014.09.001. Epub 2014 Dec 26. J Fr Ophtalmol. 2015. PMID: 25547721 Review. French.
-
Disease of the Year: Differential Diagnosis of Uveitic Macular Edema.Ocul Immunol Inflamm. 2019;27(1):72-88. doi: 10.1080/09273948.2018.1523437. Epub 2018 Oct 1. Ocul Immunol Inflamm. 2019. PMID: 30273513 Review.
-
Tocilizumab in Uveitic Macular Edema Refractory to Previous Immunomodulatory Treatment.Ocul Immunol Inflamm. 2017 Apr;25(2):215-220. doi: 10.3109/09273948.2015.1099680. Epub 2016 Jan 5. Ocul Immunol Inflamm. 2017. PMID: 26731514
-
Medical Therapy of Uveitic Macular Edema: Biologic Agents.Ocul Immunol Inflamm. 2020 Nov 16;28(8):1239-1250. doi: 10.1080/09273948.2019.1709648. Epub 2020 Feb 14. Ocul Immunol Inflamm. 2020. PMID: 32058830 Review.
-
Epidemiology of Macular Edema in Uveitis.Ocul Immunol Inflamm. 2019;27(2):169-180. doi: 10.1080/09273948.2019.1576910. Epub 2019 Mar 1. Ocul Immunol Inflamm. 2019. PMID: 30821631 Review.
Cited by
-
Correlation between Morphological Characteristics of Macular Edema and Visual Acuity in Young Patients with Idiopathic Intermediate Uveitis.Medicina (Kaunas). 2023 Mar 8;59(3):529. doi: 10.3390/medicina59030529. Medicina (Kaunas). 2023. PMID: 36984530 Free PMC article.
-
Risk factors for the development of macular edema in children with uveitis.Front Ophthalmol (Lausanne). 2023 Jun 2;3:1134077. doi: 10.3389/fopht.2023.1134077. eCollection 2023. Front Ophthalmol (Lausanne). 2023. PMID: 38983006 Free PMC article.
-
Quantitative effect of subretinal fluid and intraretinal edema on visual acuity in uveitic cystoid macular edema.J Ophthalmic Inflamm Infect. 2021 Oct 11;11(1):38. doi: 10.1186/s12348-021-00266-y. J Ophthalmic Inflamm Infect. 2021. PMID: 34635967 Free PMC article.
-
Ptosis induced by topical steroid eye drops: Two cases reports.Medicine (Baltimore). 2017 Dec;96(51):e9288. doi: 10.1097/MD.0000000000009288. Medicine (Baltimore). 2017. PMID: 29390490 Free PMC article.
-
The Impact of Oxidative Stress on Blood-Retinal Barrier Physiology in Age-Related Macular Degeneration.Cells. 2021 Jan 4;10(1):64. doi: 10.3390/cells10010064. Cells. 2021. PMID: 33406612 Free PMC article. Review.
References
-
- Gritz DC, Wong IG. Incidence and prevalence of uveitis in Northern California; the Northern California Epidemiology of Uveitis Study. Ophthalmology 2004; 111: 491–500. - PubMed
-
- Suhler EB, Lloyd MJ, Choi D, Rosenbaum JT, Austin DF. Incidence and prevalence of uveitis in Veterans Affairs Medical Centers of the Pacific Northwest. Am J Ophthalmol 2008; 146: 890–896. - PubMed
-
- Lardenoye CW, van Kooij B, Rothova A. Impact of macular edema on visual acuity in uveitis. Ophthalmology 2006; 113: 1446–1449. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
