

Impaired Pulmonary Diffusion in Heart Failure With Preserved Ejection Fraction
- PMID: 27256752
- PMCID: PMC4893169
- DOI: 10.1016/j.jchf.2016.03.001
Impaired Pulmonary Diffusion in Heart Failure With Preserved Ejection Fraction
Abstract
Objectives: The purpose of this study was to compare measures of gas exchange at rest and during exercise in patients with heart failure and preserved ejection fraction (HFpEF) with age- and sex-matched control subjects.
Background: Patients with HFpEF display elevation in left heart pressures, but it is unclear how this affects pulmonary gas transfer or its determinants at rest and during exercise.
Methods: Patients with HFpEF (n = 20) and control subjects (n = 26) completed a recumbent cycle ergometry exercise test with simultaneous measurement of ventilation and gas exchange. Diffusion of the lungs for carbon monoxide (DLCO) and its subcomponents, pulmonary capillary blood volume (VC) and alveolar-capillary membrane conductance (DM), were measured at rest, and matched for low-intensity (20 W) and peak exercise. Stroke volume was measured by transthoracic echocardiography to calculate cardiac output.
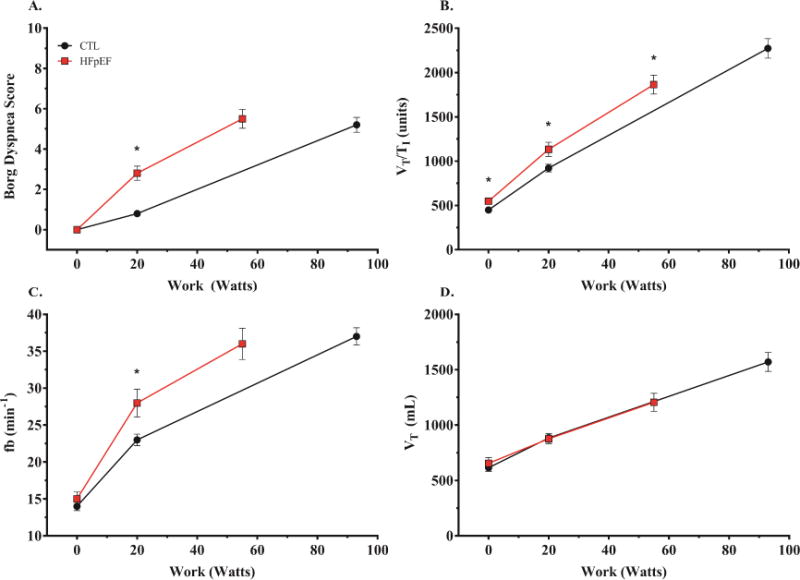
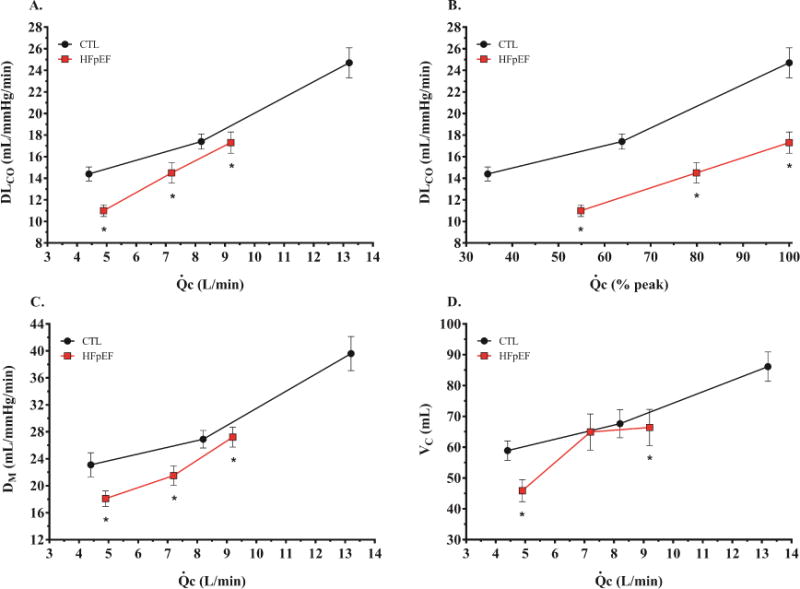
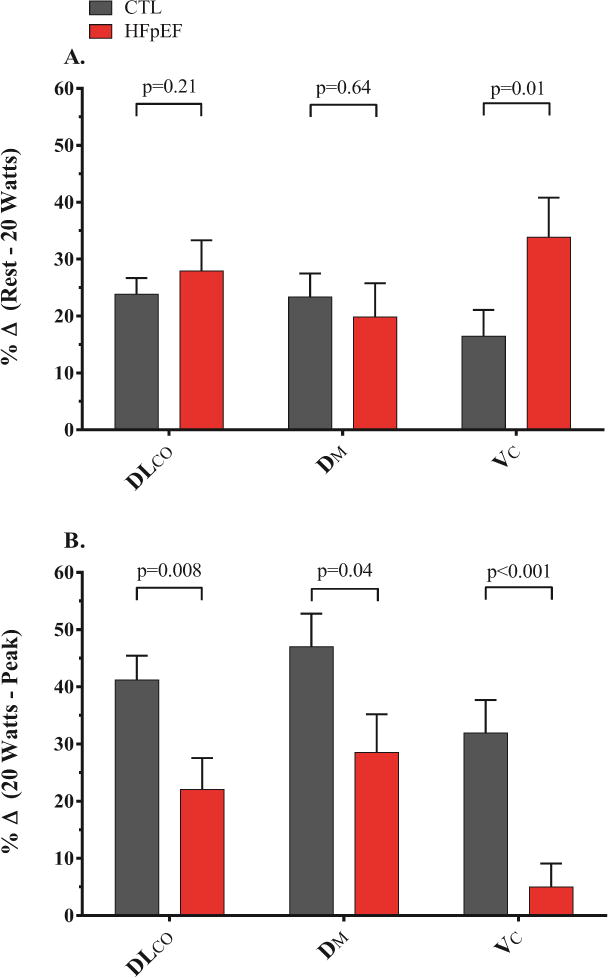
Results: Compared with control subjects, patients with HFpEF displayed impaired diastolic function and reduced exercise capacity. Patients with HFpEF demonstrated a 24% lower DLCO at rest (11.0 ± 2.3 ml/mm Hg/min vs. 14.4 ± 3.3 ml/mm Hg/min; p < 0.01) related to reductions in both DM (18.1 ± 4.9 ml/mm Hg/min vs. 23.1 ± 9.1 ml/mm Hg/min; p = 0.04), and VC (45.9 ± 15.2. ml vs. 58.9 ± 16.2 ml; p = 0.01). DLCO was lower in patients with HFpEF compared with control subjects in all stages of exercise, yet its determinants showed variable responses. With low-level exercise, patients with HFpEF demonstrated greater relative increases in VC, coupled with heightened ventilatory drive and more severe symptoms of dyspnea compared with control subjects. At 20-W exercise, DM was markedly reduced in patients with HFpEF compared with control subjects. From 20 W to peak exercise, there was no further increase in VC in patients with HFpEF, which in tandem with reduced DM, led to a 30% reduction in DLCO at peak exercise (17.3 ± 4.2 ml/mm Hg/min vs. 24.7 ± 7.1 ml/mm Hg/min; p < 0.01).
Conclusions: Subjects with HFpEF display altered pulmonary function and gas exchange at rest and especially during exercise, which contributes to exercise intolerance. Novel therapies that improve gas diffusion may be effective to improve exercise tolerance in patients with HFpEF.
Keywords: HFpEF; exercise; lung diffusion.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Impaired Alveolar Capillary Membrane Diffusion: A Recently Recognized Contributor to Exertional Dyspnea in Heart Failure With Preserved Ejection Fraction.JACC Heart Fail. 2016 Jun;4(6):499-501. doi: 10.1016/j.jchf.2016.03.020. JACC Heart Fail. 2016. PMID: 27256753 No abstract available.
References
-
- Zile MR, Baicu CF, Gaasch WH. Diastolic heart failure-abnormalities in active relaxation and passive stiffness of the left ventricle. N Engl J Med. 2004;350:1953–1959. - PubMed
-
- Westermann D, Kasner M, Steendijk P, et al. Role of left ventricular stiffness in heart failure iwth normal ejection fraction. Circulation. 2008;117:2051–2060. - PubMed
-
- Guazzi M, Borlaug BA. Pulmonary hypertension due to left heart disease. Circulation. 2012;126:975–990. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
