

Diagnosis of infant synostotic and nonsynostotic cranial deformities: a review for pediatricians
- PMID: 27256993
- PMCID: PMC5176072
- DOI: 10.1016/j.rpped.2016.01.004
Diagnosis of infant synostotic and nonsynostotic cranial deformities: a review for pediatricians
Abstract
Objective: To review the current comprehensive care for nonsyndromic craniosynostosis and nonsynostotic cranial deformity and to offer an overall view of these craniofacial conditions.
Data source: The review was conducted in the PubMed, SciELO, and LILACS databases without time or language restrictions. Relevant articles were selected for the review.
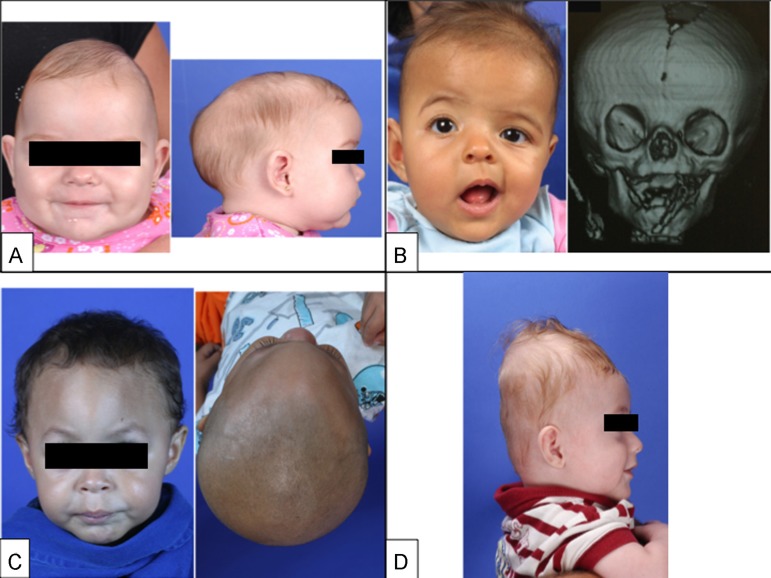
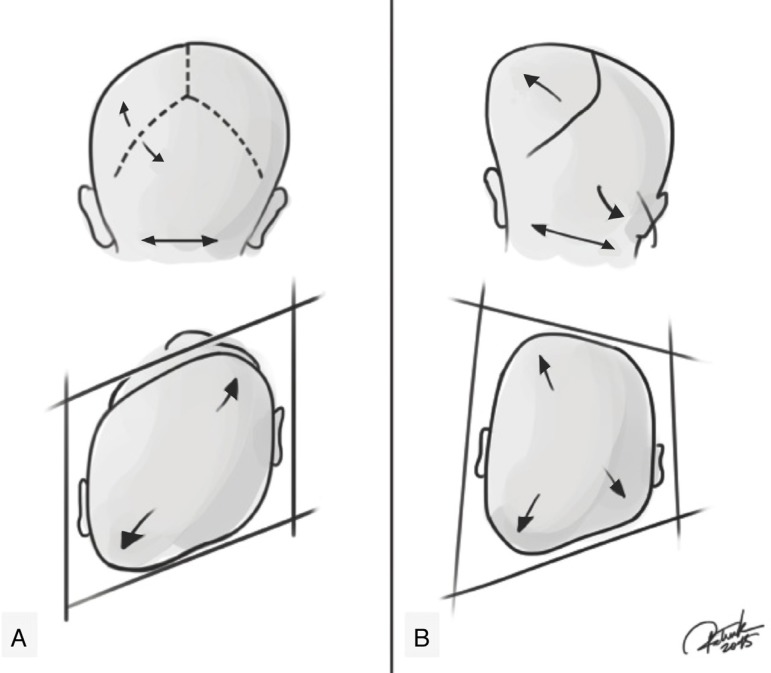
Data synthesis: We included the anatomy and physiology of normal skull development of children, discussing nuances related to nomenclature, epidemiology, etiology, and treatment of the most common forms of nonsyndromic craniosynostosis. The clinical criteria for the differential diagnosis between positional deformities and nonsyndromic craniosynostosis were also discussed, giving to the pediatrician subsidies for a quick and safe clinical diagnosis. If positional deformity is accurately diagnosed, it can be treated successfully with behavior modification. Diagnostic doubts and craniosynostosis patients should be referred straightaway to a multidisciplinary craniofacial center.
Conclusions: Pediatricians are in the forefront of the diagnosis of patients with cranial deformities. Thus, it is of paramount importance that they recognize subtle cranial deformities as it may be related to premature fusion of cranial sutures.
Objetivo:: Revisar o atendimento integral atual de craniossinostose não sindrômica e deformidade craniana não sinostótica e oferecer uma visão global dessas condições craniofaciais.
Fontes de dados:: A revisão foi feita nas bases de dados PubMed, SciELO e Lilacs e sem restrições de tempo ou idioma. Artigos relevantes foram selecionados para a revisão.
Síntese dos dados:: Foram incluídas a anatomia e a fisiologia do desenvolvimento normal do crânio em crianças, discutidas nuances relacionadas à nomenclatura, epidemiologia, etiologia e ao tratamento das formas mais comuns de craniossinostose não sindrômica. Também foram discutidos os critérios clínicos para o diagnóstico diferencial entre deformidades posicionais e craniossinostose não sindrômica. Deram-se aos pediatras subsídios para um diagnóstico clínico rápido e seguro. Se deformidades posicionais forem diagnosticadas com precisão, elas podem ser tratadas com sucesso por meio da modificação do comportamento. Dúvidas de diagnóstico e pacientes portadores de craniossinostose devem ser encaminhados imediatamente a um centro multidisciplinar craniofacial.
Conclusões:: Os pediatras estão na vanguarda do diagnóstico de pacientes com deformidades cranianas. Assim, é de suma importância que reconheçam deformidades cranianas sutis, pois elas podem estar relacionadas à fusão prematura das suturas cranianas.
Keywords: Anormalidades craniofaciais; Craniofacial abnormalities; Craniossinostose; Craniosynostosis; Diagnosis; Diagnóstico; Pediatras; Pediatricians.
Copyright © 2016 Sociedade de Pediatria de São Paulo. Publicado por Elsevier Editora Ltda. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Peitsch WK, Keefer CH, LaBrie RA, Mulliken JB. Incidence of cranial asymmetry in healthy newborns. Pediatrics. 2002;110:e72. - PubMed
-
- Furuya Y, Edwards MS, Alpers CE, Tress BM, Ousterhout DK, Norman D. Computerized tomography of cranial sutures. Part 1: comparison of suture anatomy in children and adults. J Neurosurg. 1984;61:53–58. - PubMed
-
- Slater BJ, Lenton KA, Kwan MD, Gupta DM, Wan DC, Longaker MT. Cranial sutures: a brief review. Plast Reconstr Surg. 2008;121:170e–178e. - PubMed
-
- Aviv RI, Rodger E, Hall CM. Craniosynostosis. Clin Radiol. 2002;57:93–102. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
