

Clinical development of gene therapy: results and lessons from recent successes
- PMID: 27257611
- PMCID: PMC4879992
- DOI: 10.1038/mtm.2016.34
Clinical development of gene therapy: results and lessons from recent successes
Abstract
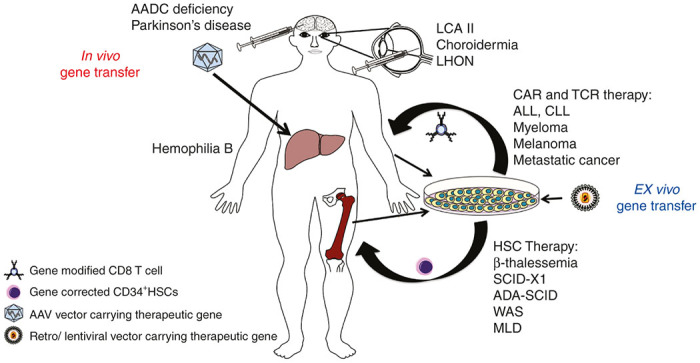
Therapeutic gene transfer holds the promise of providing lasting therapies and even cures for diseases that were previously untreatable or for which only temporary or suboptimal treatments were available. For some time, clinical gene therapy was characterized by some impressive but rare examples of successes and also several setbacks. However, effective and long-lasting treatments are now being reported from gene therapy trials at an increasing pace. Positive outcomes have been documented for a wide range of genetic diseases (including hematological, immunological, ocular, and neurodegenerative and metabolic disorders) and several types of cancer. Examples include restoration of vision in blind patients, eradication of blood cancers for which all other treatments had failed, correction of hemoglobinopathies and coagulation factor deficiencies, and restoration of the immune system in children born with primary immune deficiency. To date, about 2,000 clinical trials for various diseases have occurred or are in progress, and many more are in the pipeline. Multiple clinical studies reported successful treatments of pediatric patients. Design of gene therapy vectors and their clinical development are advancing rapidly. This article reviews some of the major successes in clinical gene therapy of recent years.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
