

Frailty as a Predictor of Acute Kidney Injury in Hospitalized Elderly Patients: A Single Center, Retrospective Cohort Study
- PMID: 27257823
- PMCID: PMC4892677
- DOI: 10.1371/journal.pone.0156444
Frailty as a Predictor of Acute Kidney Injury in Hospitalized Elderly Patients: A Single Center, Retrospective Cohort Study
Abstract
Background: Elderly patients have an increased risk for acute kidney injury (AKI). However, few studies have reported on predictors for AKI in geriatric patients. Therefore, we aimed at determining the effect of frailty as a predictor of AKI.
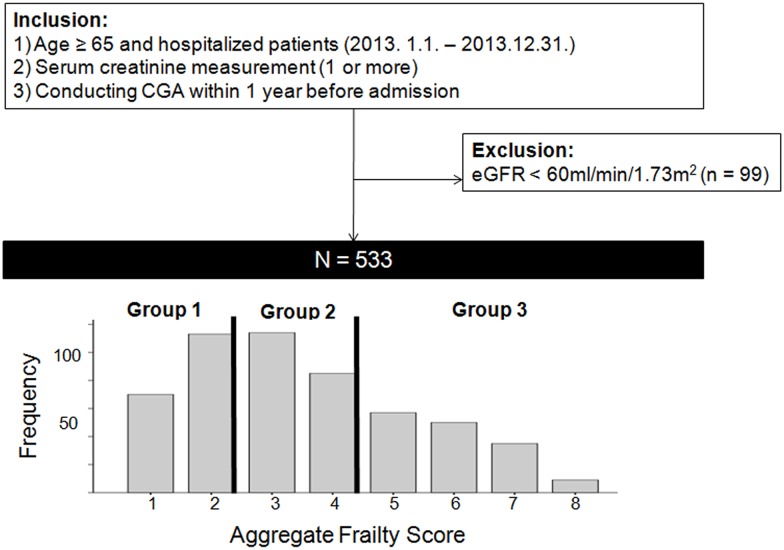
Methods: We retrospectively enrolled 533 hospitalized elderly patients (aged ≥ 65 years) who had their creatinine levels measured (≥ 1 measurement) during admission for a period of 1 year (2013) and conducted a comprehensive geriatric assessment (CGA) within 1 year before the index hospitalization. We examined five variables (activity of daily living [ADL] and instrumental ADL dependence, dementia, nutrition, and polypharmacy) from CGA. We categorized the patients into 3 groups according to the tertile of aggregate frailty scores: Group 1, score 1-2; Group 2, score 3-4; Group 3, score 5-8).
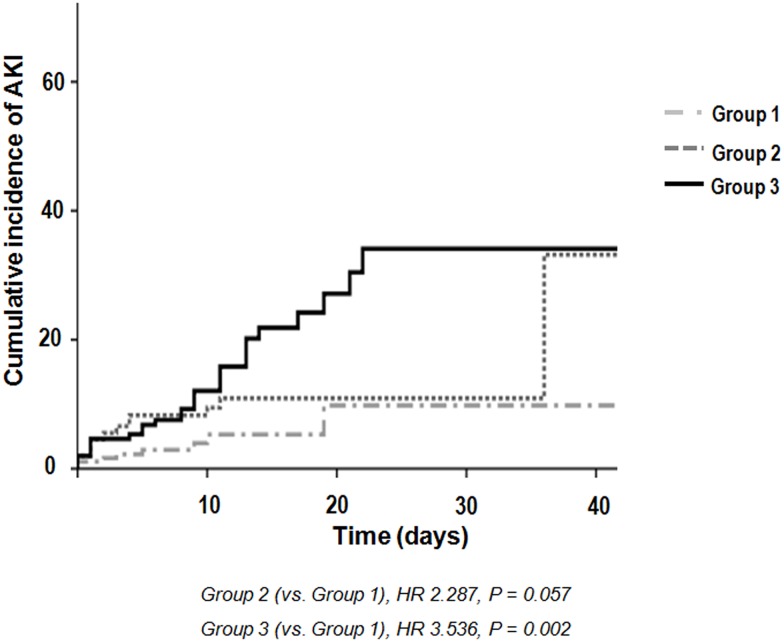
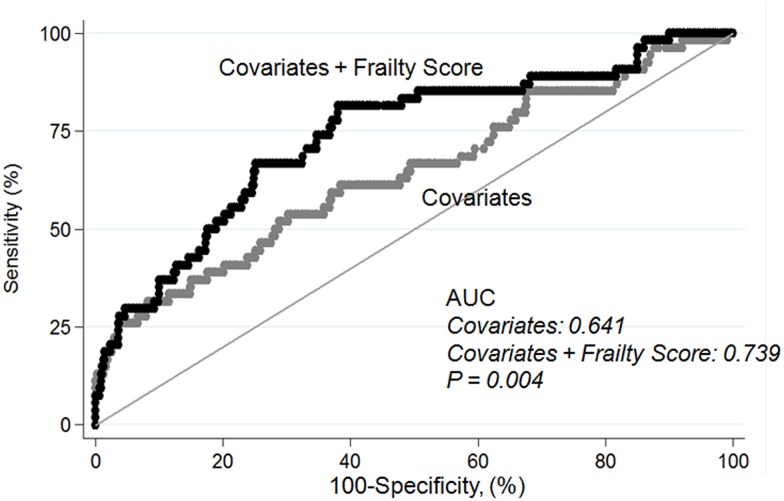
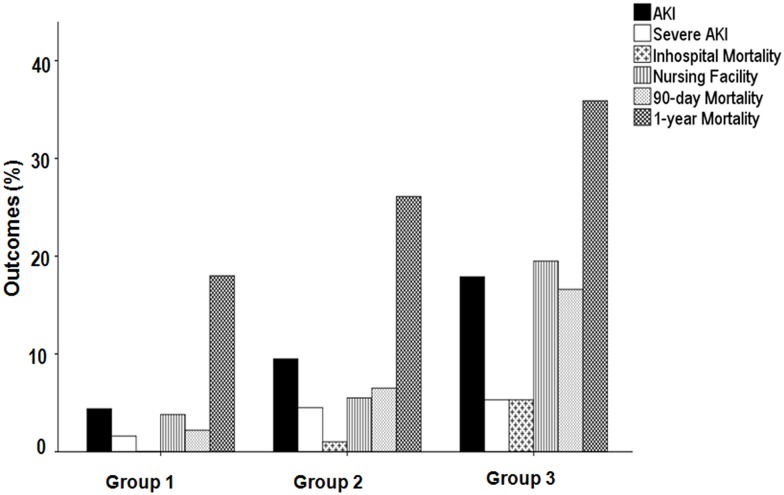
Results: Fifty-four patients (10.1%) developed AKI (median duration, 4 days). The frailest group (Group 3) showed an increased risk of AKI as compared to Group 1, (hazard ratio [HR] = 3.536, P = 0.002). We found that discriminatory accuracy for AKI improved with the addition of the tertile of aggregate frailty score to covariates (area under the receiver operator characteristics curves [AUROC] 0.641, AUROC 0.739, P = 0.004). Forty-six patients (8.6%) were transferred to nursing facilities and 477 patients (89.5%) were discharged home. The overall 90-day and 1-year mortality for elderly inpatients were 7.9% and 26.3%. The frailest group also demonstrated an increased risk of discharge to nursing facilities, and 90-day and 1-year mortality as compared to Group 1, independent of AKI severity (nursing facilities: odd ratio = 4.843, P = 0.002; 90-day mortality: HR = 6.555, P = 0.002; 1-year mortality: HR = 3.249, P = 0.001).
Conclusions: We found that frailty may independently predict the development of AKI and adverse outcomes in geriatric inpatients.
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
