

Mindfulness-based stress reduction and cognitive behavioral therapy for chronic low back pain: similar effects on mindfulness, catastrophizing, self-efficacy, and acceptance in a randomized controlled trial
- PMID: 27257859
- PMCID: PMC5069124
- DOI: 10.1097/j.pain.0000000000000635
Mindfulness-based stress reduction and cognitive behavioral therapy for chronic low back pain: similar effects on mindfulness, catastrophizing, self-efficacy, and acceptance in a randomized controlled trial
Abstract
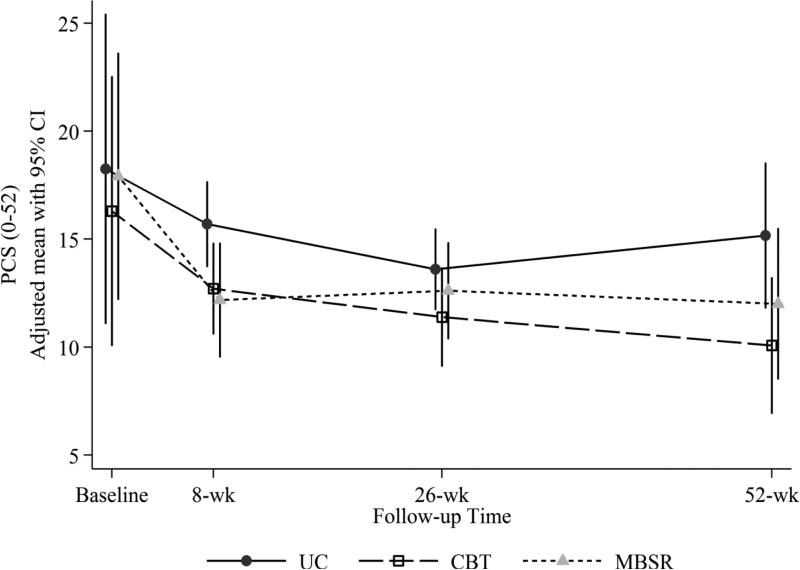
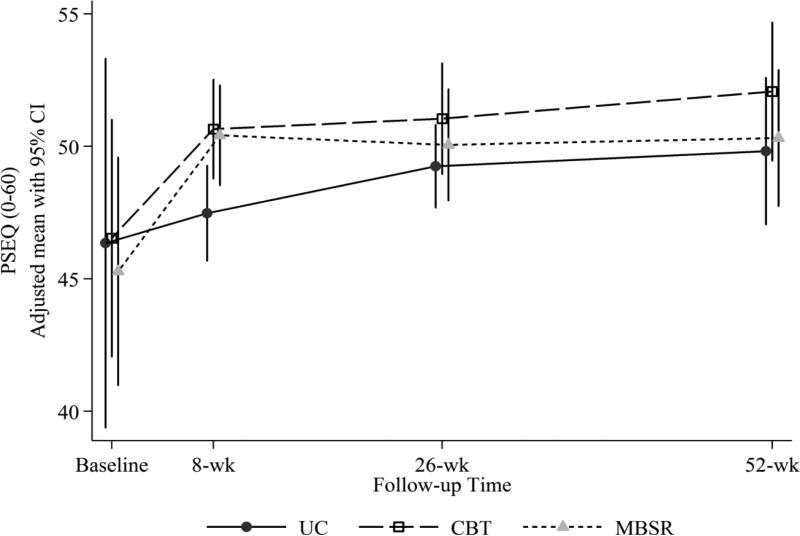
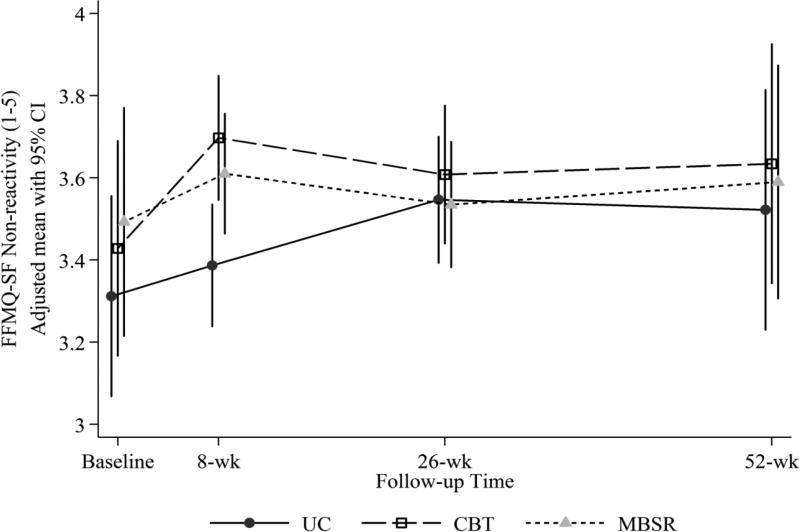
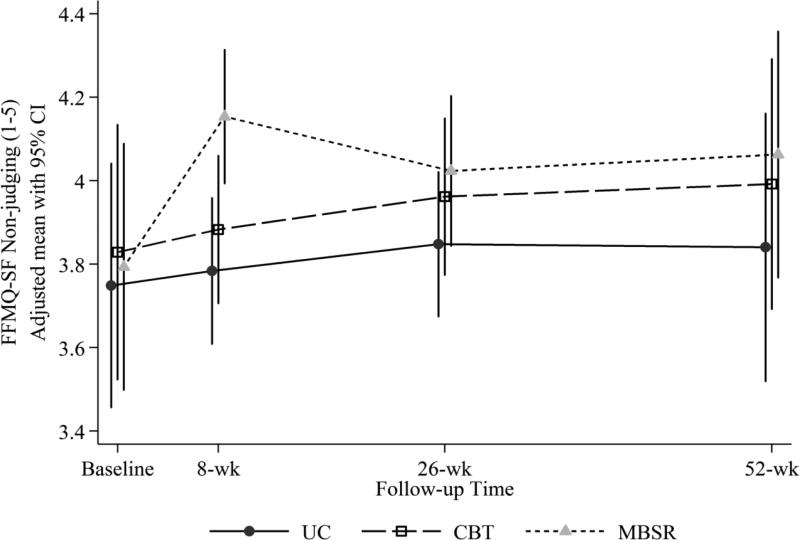
Cognitive behavioral therapy (CBT) is believed to improve chronic pain problems by decreasing patient catastrophizing and increasing patient self-efficacy for managing pain. Mindfulness-based stress reduction (MBSR) is believed to benefit patients with chronic pain by increasing mindfulness and pain acceptance. However, little is known about how these therapeutic mechanism variables relate to each other or whether they are differentially impacted by MBSR vs CBT. In a randomized controlled trial comparing MBSR, CBT, and usual care (UC) for adults aged 20 to 70 years with chronic low back pain (N = 342), we examined (1) baseline relationships among measures of catastrophizing, self-efficacy, acceptance, and mindfulness and (2) changes on these measures in the 3 treatment groups. At baseline, catastrophizing was associated negatively with self-efficacy, acceptance, and 3 aspects of mindfulness (nonreactivity, nonjudging, and acting with awareness; all P values <0.01). Acceptance was associated positively with self-efficacy (P < 0.01) and mindfulness (P values <0.05) measures. Catastrophizing decreased slightly more posttreatment with MBSR than with CBT or UC (omnibus P = 0.002). Both treatments were effective compared with UC in decreasing catastrophizing at 52 weeks (omnibus P = 0.001). In both the entire randomized sample and the subsample of participants who attended ≥6 of the 8 MBSR or CBT sessions, differences between MBSR and CBT at up to 52 weeks were few, small in size, and of questionable clinical meaningfulness. The results indicate overlap across measures of catastrophizing, self-efficacy, acceptance, and mindfulness and similar effects of MBSR and CBT on these measures among individuals with chronic low back pain.
Figures
Comment in
-
Mechanisms, mechanisms, mechanisms: it really does all boil down to mechanisms.Pain. 2016 Nov;157(11):2393-2394. doi: 10.1097/j.pain.0000000000000696. Pain. 2016. PMID: 27548048 Free PMC article. No abstract available.
References
-
- Åkerblom S, Perrin S, Rivano Fischer M, McCracken LM. The mediating role of acceptance in multidisciplinary cognitive-behavioral therapy for chronic pain. J Pain. 16(7):606–615. - PubMed
-
- Baranoff J, Hanrahan SJ, Kapur D, Connor JP. Acceptance as a process variable in relation to catastrophizing in multidisciplinary pain treatment. Eur J Pain. 2013;17(1):101–110. - PubMed
-
- Bernardy K, Fuber N, Kollner V, Hauser W. Efficacy of cognitive-behavioral therapies in fibromyalgia syndrome — a systematic review and metaanalysis of randomized controlled trials. J Rheumatol. 2010;37(10):1991–2005. - PubMed
-
- Blacker M, Meleo-Meyer F, Kabat-Zinn J, Santorelli SF. Stress Reduction Clinic Mindfulness-Based Stress Reduction (MBSR) Curriculum Guide. Center for Mindfulness in Medicine, Health Care, and Society, Division of Preventive and Behavioral Medicine, Department of Medicine, University of Massachusetts Medical School; Worcester, MA: 2009.
-
- Bohlmeijer E, ten Klooster P, Fledderus M, Veehof M, Baer R. Psychometric properties of the five facet mindfulness questionnaire in depressed adults and development of a short form. Assessment. 2011;18:308–320. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
