

sFlt Multivalent Conjugates Inhibit Angiogenesis and Improve Half-Life In Vivo
- PMID: 27257918
- PMCID: PMC4892585
- DOI: 10.1371/journal.pone.0155990
sFlt Multivalent Conjugates Inhibit Angiogenesis and Improve Half-Life In Vivo
Abstract
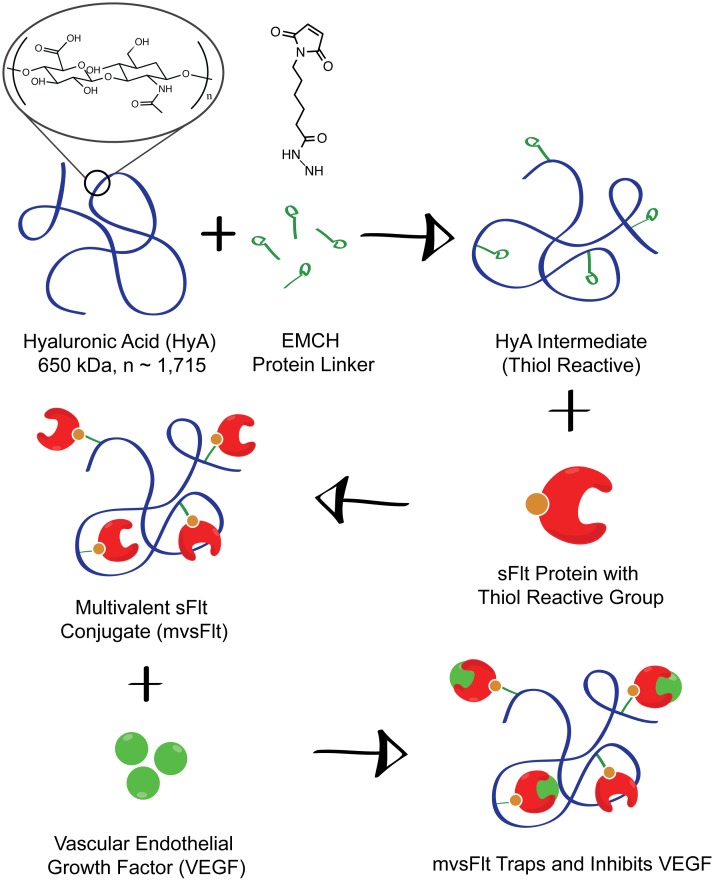
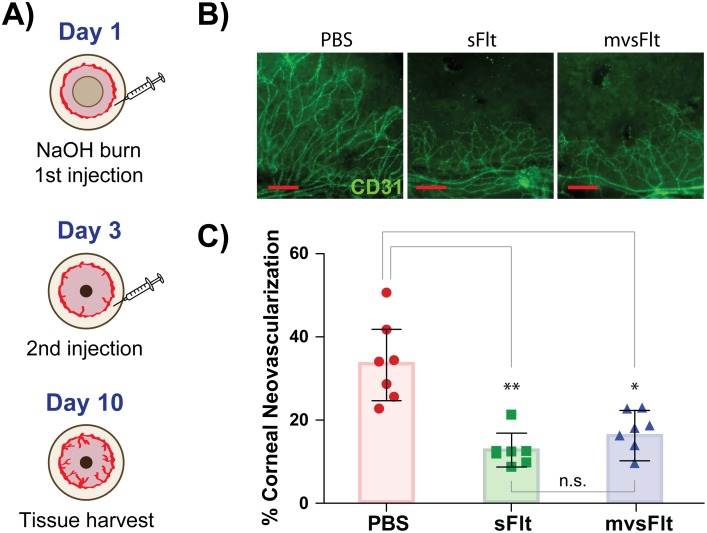
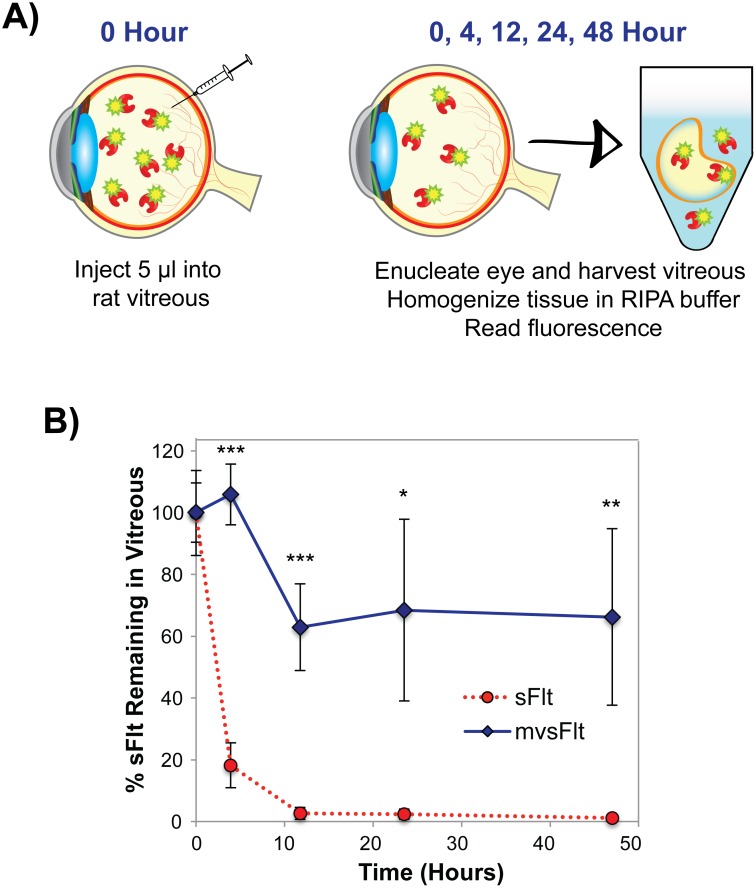
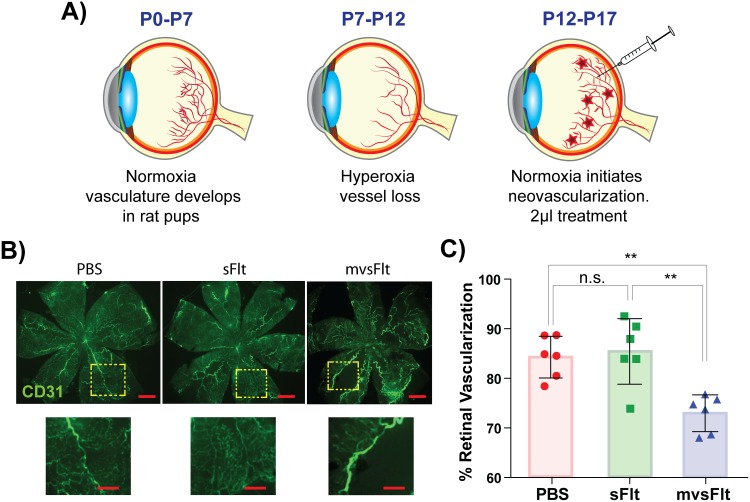
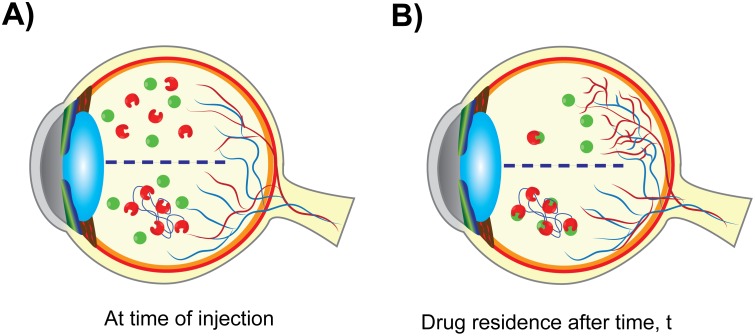
Current anti-VEGF drugs for patients with diabetic retinopathy suffer from short residence time in the vitreous of the eye. In order to maintain biologically effective doses of drug for inhibiting retinal neovascularization, patients are required to receive regular monthly injections of drug, which often results in low patient compliance and progression of the disease. To improve the intravitreal residence time of anti-VEGF drugs, we have synthesized multivalent bioconjugates of an anti-VEGF protein, soluble fms-like tyrosine kinase-1 (sFlt) that is covalently grafted to chains of hyaluronic acid (HyA), conjugates that are termed mvsFlt. Using a mouse corneal angiogenesis assay, we demonstrate that covalent conjugation to HyA chains does not decrease the bioactivity of sFlt and that mvsFlt is equivalent to sFlt at inhibiting corneal angiogenesis. In a rat vitreous model, we observed that mvsFlt had significantly increased intravitreal residence time compared to the unconjugated sFlt after 2 days. The calculated intravitreal half-lives for sFlt and mvsFlt were 3.3 and 35 hours, respectively. Furthermore, we show that mvsFlt is more effective than the unconjugated form at inhibiting retinal neovascularization in an oxygen-induced retinopathy model, an effect that is most likely due to the longer half-life of mvsFlt in the vitreous. Taken together, our results indicate that conjugation of sFlt to HyA does not affect its affinity for VEGF and this conjugation significantly improves drug half-life. These in vivo results suggest that our strategy of multivalent conjugation could substantially improve upon drug half-life, and thus the efficacy of currently available drugs that are used in diseases such as diabetic retinopathy, thereby improving patient quality of life.
Conflict of interest statement
Figures
Similar articles
-
Multivalent hyaluronic acid bioconjugates improve sFlt-1 activity in vitro.Biomaterials. 2016 Jul;93:95-105. doi: 10.1016/j.biomaterials.2016.03.017. Epub 2016 Mar 12. Biomaterials. 2016. PMID: 27086270 Free PMC article.
-
Preclinical and phase 1A clinical evaluation of an anti-VEGF pegylated aptamer (EYE001) for the treatment of exudative age-related macular degeneration.Retina. 2002 Apr;22(2):143-52. doi: 10.1097/00006982-200204000-00002. Retina. 2002. PMID: 11927845 Clinical Trial.
-
Plasma VEGF and soluble VEGF receptor FLT-1 in proliferative retinopathy: relationship to endothelial dysfunction and laser treatment.Invest Ophthalmol Vis Sci. 2000 Jul;41(8):2115-9. Invest Ophthalmol Vis Sci. 2000. PMID: 10892852
-
Anti-Flt1 peptide - hyaluronate conjugate for the treatment of retinal neovascularization and diabetic retinopathy.Biomaterials. 2011 Apr;32(11):3115-23. doi: 10.1016/j.biomaterials.2011.01.003. Epub 2011 Jan 28. Biomaterials. 2011. PMID: 21277020
-
Marked inhibition of retinal neovascularization in rats following soluble-flt-1 gene transfer.J Gene Med. 2004 Sep;6(9):992-1002. doi: 10.1002/jgm.586. J Gene Med. 2004. PMID: 15352072
Cited by
-
Synthesis and Characterization of Novel Succinyl Chitosan-Dexamethasone Conjugates for Potential Intravitreal Dexamethasone Delivery.Int J Mol Sci. 2021 Oct 11;22(20):10960. doi: 10.3390/ijms222010960. Int J Mol Sci. 2021. PMID: 34681619 Free PMC article.
-
Polysaccharides in Ocular Drug Delivery.Pharmaceutics. 2019 Dec 24;12(1):22. doi: 10.3390/pharmaceutics12010022. Pharmaceutics. 2019. PMID: 31878298 Free PMC article. Review.
-
Multivalent conjugates of basic fibroblast growth factor enhance in vitro proliferation and migration of endothelial cells.Biomater Sci. 2018 May 1;6(5):1076-1083. doi: 10.1039/c7bm01052d. Biomater Sci. 2018. PMID: 29595848 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
