

Effects of Microwave Ablation on Arterial and Venous Vasculature after Treatment of Hepatocellular Carcinoma
- PMID: 27257951
- PMCID: PMC5084967
- DOI: 10.1148/radiol.2016152508
Effects of Microwave Ablation on Arterial and Venous Vasculature after Treatment of Hepatocellular Carcinoma
Abstract
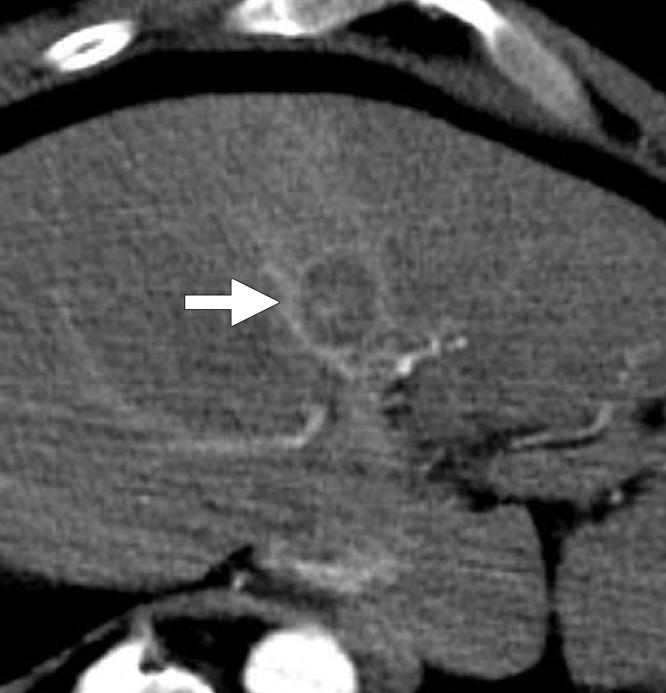
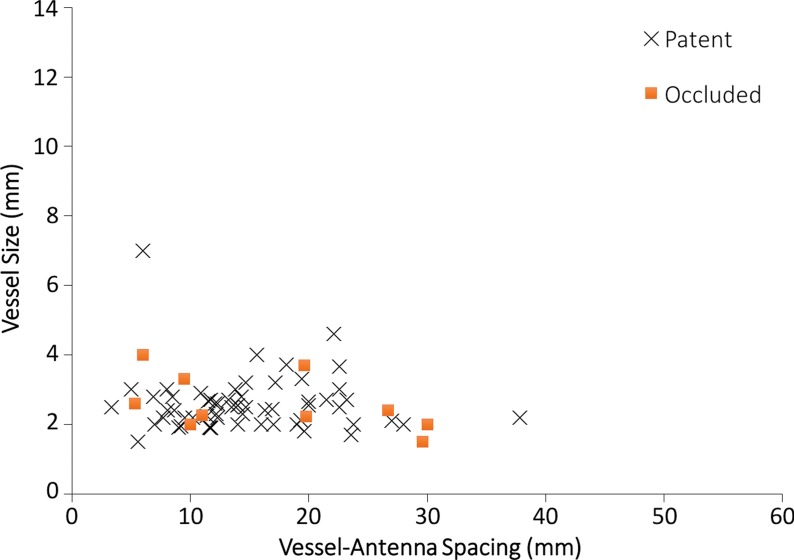
Purpose To characterize vessel occlusion rates and their role in local tumor progression in patients with hepatocellular carcinoma (HCC) who underwent microwave tumor ablation. Materials and Methods This institutional review board approved, HIPAA-compliant retrospective review included 95 patients (75 men and 20 women) with 124 primary HCCs who were treated at a single center between January 2011 and March 2014. Complete occlusion of the portal veins, hepatic veins, and hepatic arteries within and directly abutting the ablation zone was identified with postprocedure contrast material-enhanced computed tomography. For each vessel identified in the ablation zone, its size and antenna spacing were recorded and correlated with vascular occlusion with logistic regression analysis. Local tumor progression rates were then compared between patent and occluded vessels for each vessel type with Fisher exact test. Results Occlusion was identified in 39.7% of portal veins (29 of 73), 15.0% of hepatic veins (six of 40), and 14.2% of hepatic arteries (10 of 70) encompassed within the ablation zone. Hepatic vein occlusion was significantly correlated with a smaller vessel size (P = .036) and vessel-antenna spacing (P = .006). Portal vein occlusion was only significantly correlated with a smaller vessel size (P = .001), particularly in vessels that were less than 3 mm in diameter. Local tumor progression rates were significantly correlated with patent hepatic arteries within the ablation zone (P = .02) but not with patent hepatic (P = .57) or portal (P = .14) veins. Conclusion During microwave ablation of HCC, hepatic veins and arteries were resistant to vessel occlusion compared with portal veins, and only arterial patency within an ablation zone was related to local tumor progression. © RSNA, 2016.
Figures



References
-
- European Association For The Study Of The Liver; European Organisation For Research And Treatment Of Cancer . EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 2012;56(4):908–943. - PubMed
-
- Bhardwaj N, Strickland AD, Ahmad F, Atanesyan L, West K, Lloyd DM. A comparative histological evaluation of the ablations produced by microwave, cryotherapy and radiofrequency in the liver. Pathology 2009;41(2):168–172. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
