

Racial Disparities in Treatment Rates for Chronic Hepatitis C: Analysis of a Population-Based Cohort of 73,665 Patients in the United States
- PMID: 27258498
- PMCID: PMC4900706
- DOI: 10.1097/MD.0000000000003719
Racial Disparities in Treatment Rates for Chronic Hepatitis C: Analysis of a Population-Based Cohort of 73,665 Patients in the United States
Abstract
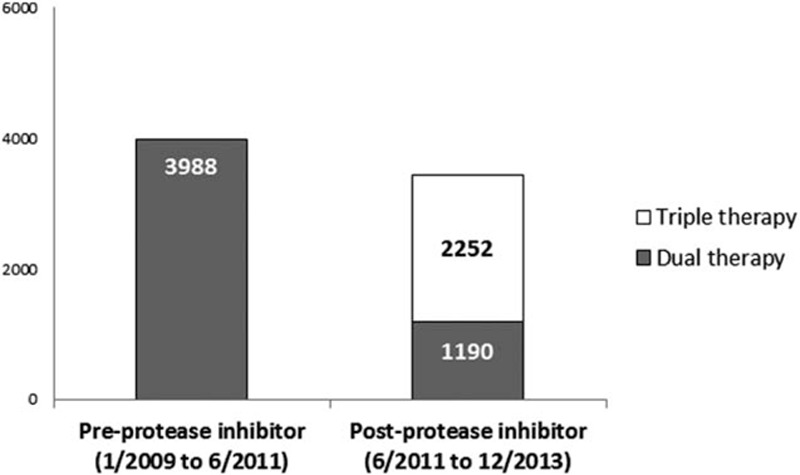
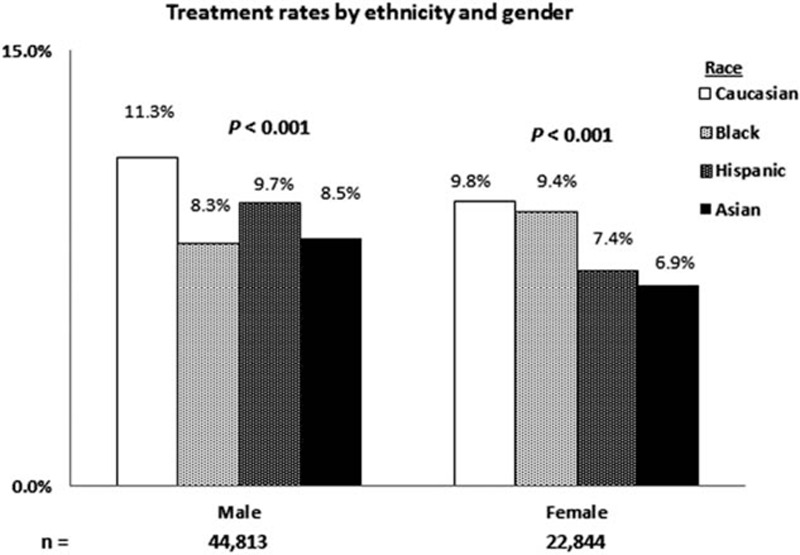
Chronic hepatitis C (CHC) disproportionately affects racial minorities in the United States (US). Although prior studies have reported lower treatment rates in Blacks than in Caucasians, the rates of other minorities remain understudied. We aimed to examine antiviral treatment rates by race and to evaluate the effect of other demographic, medical, and psychiatric factors on treatment rates. We performed a population-based study of adult CHC patients identified via ICD-9CM query from OptumInsight's Data Mart from January 2009 to December 2013. Antiviral treatment was defined by pharmaceutical claims for interferon and/or pegylated-interferon. A total of 73,665 insured patients were included: 51,282 Caucasians, 10,493 Blacks, 8679 Hispanics, and 3211 Asians. Caucasians had the highest treatment rate (10.7%) followed by Blacks (8.8%), Hispanics (8.8%), and Asians (7.9%, P < .001). Hispanics had the highest cirrhosis rates compared with Caucasians, Blacks, and Asians (20.7% vs 18.3%, 17.1%, and 14.3%, respectively). Caucasians were the most likely to have a psychiatric comorbidity (20.1%) and Blacks the most likely to have a medical comorbidity (44%). Asians were the least likely to have a psychiatric (6.4%) or medical comorbidity (26.9%). On multivariate analysis, racial minority was a significant predictor of nontreatment with odds ratios of 0.82 [confidence interval (CI): 0.74-0.90] for Blacks, 0.87 (CI: 0.78-0.96) for Hispanics, and 0.73 (CI: 0.62-0.86) for Asians versus Caucasians. Racial minorities had lower treatment rates than Caucasians. Despite fewer medical and psychiatric comorbidities and higher incomes and educational levels, Asians had the lowest treatment rates. Hispanics also had lower treatment rates than Caucasians despite having higher rates of cirrhosis. Future studies should aim to identify underlying racial-related barriers to hepatitis C virus treatment besides socioeconomic status and medical or psychiatric comorbidities.
Conflict of interest statement
P.V., J.H., and N.H.N. have no conflicts of interests to disclose.
Figures
Similar articles
-
Gender and Racial Disparities in Initial Hemodialysis Access and Outcomes in Incident End-Stage Renal Disease Patients.Am J Nephrol. 2018;48(1):4-14. doi: 10.1159/000490624. Epub 2018 Jul 10. Am J Nephrol. 2018. PMID: 29990994 Free PMC article.
-
The prevalence, burden, and treatment of severe, frequent, and migraine headaches in US minority populations: statistics from National Survey studies.Headache. 2015 Feb;55(2):214-28. doi: 10.1111/head.12506. Epub 2015 Feb 3. Headache. 2015. PMID: 25644596 Review.
-
Race/ethnicity-specific disparities in cancer incidence, burden of disease, and overall survival among patients with hepatocellular carcinoma in the United States.Cancer. 2016 Aug 15;122(16):2512-23. doi: 10.1002/cncr.30103. Epub 2016 May 19. Cancer. 2016. PMID: 27195481
-
Determinants of racial/ethnic colorectal cancer screening disparities.Arch Intern Med. 2008 Jun 23;168(12):1317-24. doi: 10.1001/archinte.168.12.1317. Arch Intern Med. 2008. PMID: 18574089
-
Long term trends and racial/ethnic disparities in the prevalence of obesity.J Community Health. 2014 Dec;39(6):1150-60. doi: 10.1007/s10900-014-9870-6. J Community Health. 2014. PMID: 24715435
Cited by
-
The U. S. Department of Veterans Affairs (VA) as a model for stronger public health infrastructure to combat HCV and other infectious diseases and reduce disparities.EClinicalMedicine. 2020 May 22;22:100391. doi: 10.1016/j.eclinm.2020.100391. eCollection 2020 May. EClinicalMedicine. 2020. PMID: 32478316 Free PMC article. No abstract available.
-
Barriers to care for chronic hepatitis C in the direct-acting antiviral era: a single-centre experience.BMJ Open Gastroenterol. 2017 Dec 20;4(1):e000181. doi: 10.1136/bmjgast-2017-000181. eCollection 2017. BMJ Open Gastroenterol. 2017. PMID: 29333275 Free PMC article.
-
Race and Hepatitis C Care Continuum in an Underserved Birth Cohort.J Gen Intern Med. 2019 Oct;34(10):2005-2013. doi: 10.1007/s11606-018-4649-6. Epub 2018 Sep 20. J Gen Intern Med. 2019. PMID: 30238404 Free PMC article.
-
Assessing health-related resiliency in HIV+ Latin women: Preliminary psychometric findings.PLoS One. 2017 Jul 19;12(7):e0181253. doi: 10.1371/journal.pone.0181253. eCollection 2017. PLoS One. 2017. PMID: 28723939 Free PMC article.
-
Self-awareness of hepatitis C infection in the United States: A cross-sectional study based on the National Health Nutrition and Examination Survey.PLoS One. 2023 Oct 24;18(10):e0293315. doi: 10.1371/journal.pone.0293315. eCollection 2023. PLoS One. 2023. PMID: 37874815 Free PMC article.
References
-
- 1998; Di Bisceglie AM, Hepatitis C. Lancet. 351:351–355. - PubMed
-
- Armstrong GL, Wasley A, Simard EP, et al. The prevalence of hepatitis C virus infection in the United States, 1999 through 2002. Ann Intern Med 2006; 144:705–714. - PubMed
-
- Dev A, Sundararajan V, Sievert W. Ethnic and cultural determinants influence risk assessment for hepatitis C acquisition. J Gastroenterol Hepatol 2004; 19:792–798. - PubMed
-
- Ho EY, Ha NB, Ahmed A, et al. Prospective study of risk factors for hepatitis C virus acquisition by Caucasian, Hispanic, and Asian American patients. J Viral Hepat 2012; 19:e105–e111. - PubMed
-
- Kin KC, Lin B, Chaung KT, et al. Less-established risk factors are common in Asian Americans with hepatitis C virus: a case-controlled study. Dig Dis Sci 2013; 58:3342–3347. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
