

Rate and complications of adult epilepsy surgery in North America: Analysis of multiple databases
- PMID: 27259069
- PMCID: PMC5260847
- DOI: 10.1016/j.eplepsyres.2016.05.001
Rate and complications of adult epilepsy surgery in North America: Analysis of multiple databases
Abstract
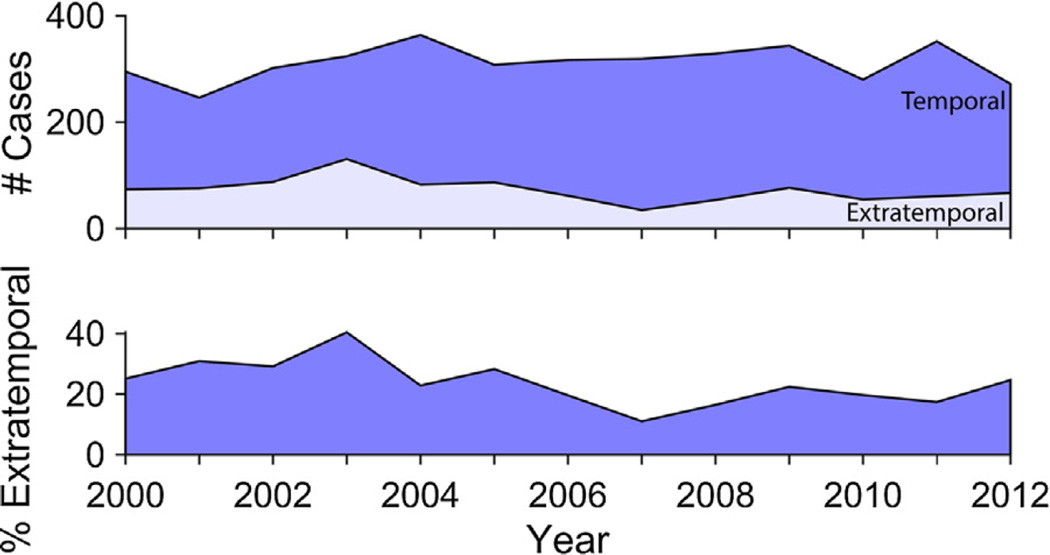
Epilepsy surgery is under-utilized, but recent studies reach conflicting conclusions regarding whether epilepsy surgery rates are currently declining, increasing, or remaining steady. However, data in these prior studies are biased toward high-volume epilepsy centers, or originate from sources that do not disaggregate various procedure types. All major epilepsy surgery procedures were extracted from the Centers for Medicare and Medicaid Services Part B National Summary Data File and the American College of Surgeons National Surgical Quality Improvement Program. Procedure rates, trends, and complications were analyzed, and patient-level predictors of postoperative adverse events were identified. Between 2000-2013, 6200 cases of epilepsy surgery were identified. Temporal lobectomy was the most common procedure (59% of cases), and most did not utilize electrocorticography (63-64%). Neither temporal nor extratemporal lobe epilepsy surgery rates changed significantly during the study period, suggesting no change in utilization. Adverse events, including major and minor complications, occurred in 15.3% of temporal lobectomies and 55.6% of hemispherectomies. Our findings suggest stagnant rates of both temporal and extratemporal lobe epilepsy surgery across U.S. surgical centers over the past decade. This finding contrasts with prior reports suggesting a recent dramatic decline in temporal lobectomy rates at high-volume epilepsy centers. We also observed higher rates of adverse events when both low- and high-volume centers were examined together, as compared to reports from high-volume centers alone. This is consistent with the presence of a volume-outcome relationship in epilepsy surgery.
Keywords: Complications; Demographics; Epilepsy; Epilepsy surgery; Seizures; Temporal lobectomy.
Copyright © 2016 Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Thirty-day non-seizure outcomes following temporal lobectomy for adult epilepsy.Clin Neurol Neurosurg. 2017 Sep;160:12-18. doi: 10.1016/j.clineuro.2017.05.027. Epub 2017 Jun 8. Clin Neurol Neurosurg. 2017. PMID: 28618390
-
Complications of epilepsy surgery in Sweden 1996-2010: a prospective, population-based study.J Neurosurg. 2015 Mar;122(3):519-25. doi: 10.3171/2014.9.JNS132679. Epub 2014 Oct 31. J Neurosurg. 2015. PMID: 25361484
-
Relationship between hospital surgical volume, lobectomy rates, and adverse perioperative events at US epilepsy centers.J Neurosurg. 2013 Jan;118(1):169-74. doi: 10.3171/2012.9.JNS12776. Epub 2012 Oct 26. J Neurosurg. 2013. PMID: 23101453
-
Trends in epilepsy surgery: stable surgical numbers despite increasing presurgical volumes.J Neurol Neurosurg Psychiatry. 2016 Dec;87(12):1322-1329. doi: 10.1136/jnnp-2016-313831. Epub 2016 Oct 5. J Neurol Neurosurg Psychiatry. 2016. PMID: 27707870 Review.
-
Current management and surgical outcomes of medically intractable epilepsy.Clin Neurol Neurosurg. 2013 Dec;115(12):2411-8. doi: 10.1016/j.clineuro.2013.09.035. Epub 2013 Oct 11. Clin Neurol Neurosurg. 2013. PMID: 24169149 Review.
Cited by
-
Closed-Loop Brain Stimulation and Paradigm Shifts in Epilepsy Surgery.Neurol Clin. 2022 May;40(2):355-373. doi: 10.1016/j.ncl.2021.12.002. Epub 2022 Mar 31. Neurol Clin. 2022. PMID: 35465880 Free PMC article. Review.
-
Long-term outcome of unilateral deep brain stimulation of the subthalamic nucleus for a patient with drug-resistant focal myoclonic seizure.Ann Transl Med. 2020 Jan;8(1):18. doi: 10.21037/atm.2019.12.43. Ann Transl Med. 2020. PMID: 32055609 Free PMC article.
-
Deep learning on brief interictal intracranial recordings can accurately characterize seizure onset zones.Epilepsia. 2025 May 27:10.1111/epi.18478. doi: 10.1111/epi.18478. Online ahead of print. Epilepsia. 2025. PMID: 40423629
-
Status of epilepsy care delivery and referral in clinics, hospitals, and epilepsy centers in Japan: A nationwide survey.Epilepsia Open. 2024 Feb;9(1):314-324. doi: 10.1002/epi4.12874. Epub 2023 Dec 9. Epilepsia Open. 2024. PMID: 38044839 Free PMC article.
-
Neurosurgical Patients as Human Research Subjects: Ethical Considerations in Intracranial Electrophysiology Research.Neurosurgery. 2018 Jul 1;83(1):29-37. doi: 10.1093/neuros/nyx361. Neurosurgery. 2018. PMID: 28973530 Free PMC article. Review.
References
-
- Behrens E, Schramm J, Zentner J, König R. Surgical and neurological complications in a series of 708 epilepsy surgery procedures. Neurosurgery. 1997;41:1–9. discussion 9–10. - PubMed
-
- Berger MS, Ghatan S, Haglund MM, Dobbins J, Ojemann GA. Low-grade gliomas associated with intractable epilepsy: seizure outcome utilizing electrocorticography during tumor resection. J. Neurosurg. 1993;79:62–69. - PubMed
-
- Davies JM, Ozpinar A, Lawton MT. Volume-outcome relationships in neurosurgery. Neurosurg. Clin. N. Am. 2015;26 http://dx.doi.org/10.1016/j.nec.2014.11.015,207-18-viii. - DOI - PubMed
-
- Engel J, Wiebe S, French J, Sperling M, Williamson P, Spencer D, Gumnit R, Zahn C, Westbrook E, Enos B. Quality Standards Subcommittee of the American Academy of Neurology, American Epilepsy Society, American Association of Neurological Surgeons, Practice parameter: temporal lobe and localized neocortical resections for epilepsy: report of the Quality Standards Subcommittee of the American Academy of Neurology, in association with the American Epilepsy Society and the American Association of Neurological Surgeons. Neurology. 2003 http://dx.doi.org/10.1212/01,WNL.0000055086.35806.2D. - DOI - PubMed
-
- Engel J, McDermott MP, Wiebe S, Langfitt JT, Stern JM, Dewar S, Sperling MR, Gardiner I, Erba G, Fried I, Jacobs M, Vinters HV, Mintzer S, Kieburtz K Early Randomized Surgical Epilepsy Trial (ERSET) Study Group. Early surgical therapy for drug-resistant temporal lobe epilepsy: a randomized trial. JAMA. 2012;307:922–930. http://dx.doi.org/10.1001/jama.2012.220. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
