

Noninvasive Failure Load Prediction of Vertebrae with Simulated Lytic Defects and Biomaterial Augmentation
- PMID: 27260559
- PMCID: PMC4991609
- DOI: 10.1089/ten.TEC.2016.0078
Noninvasive Failure Load Prediction of Vertebrae with Simulated Lytic Defects and Biomaterial Augmentation
Abstract
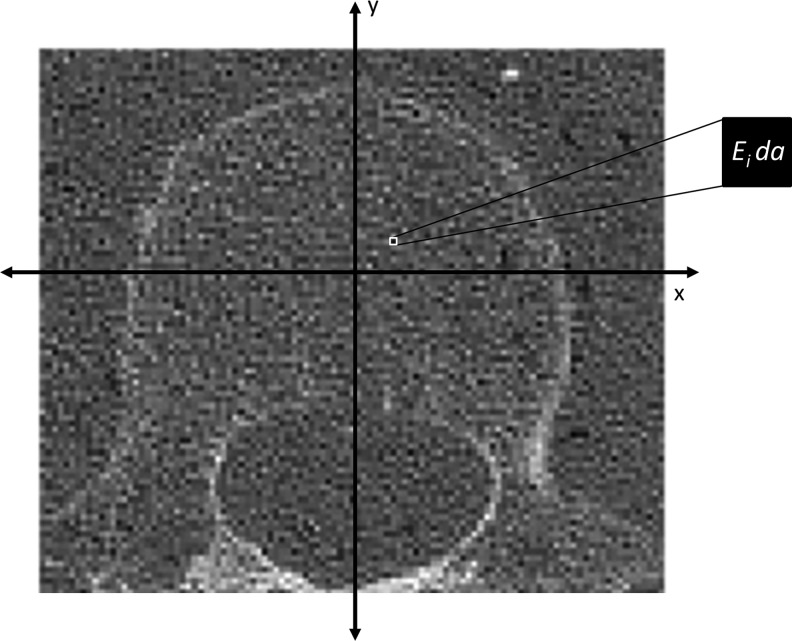
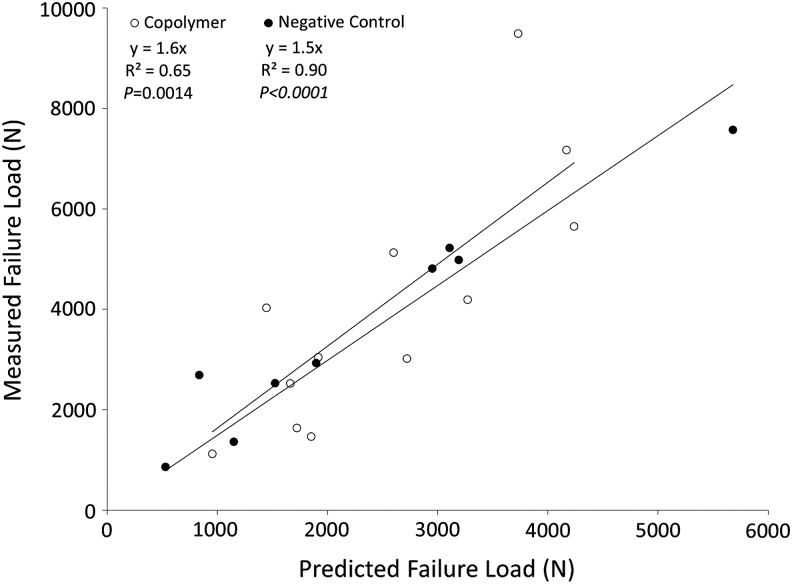
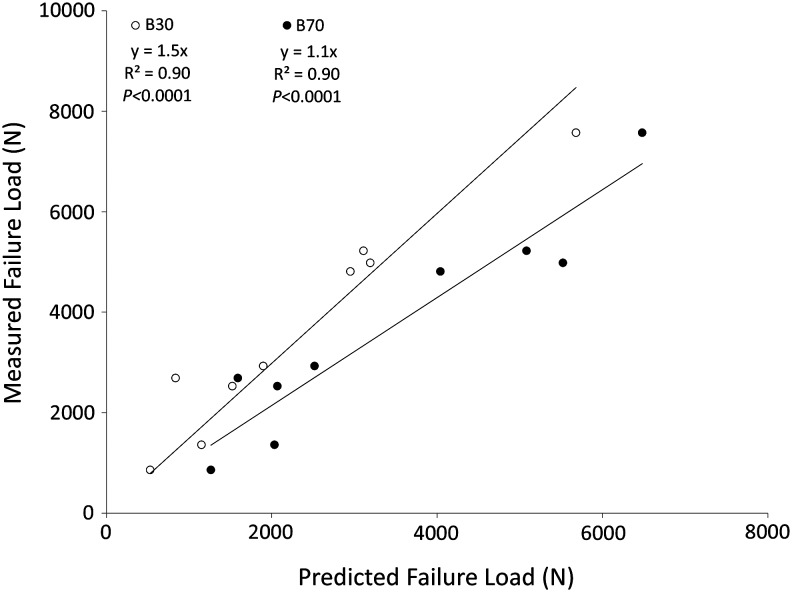
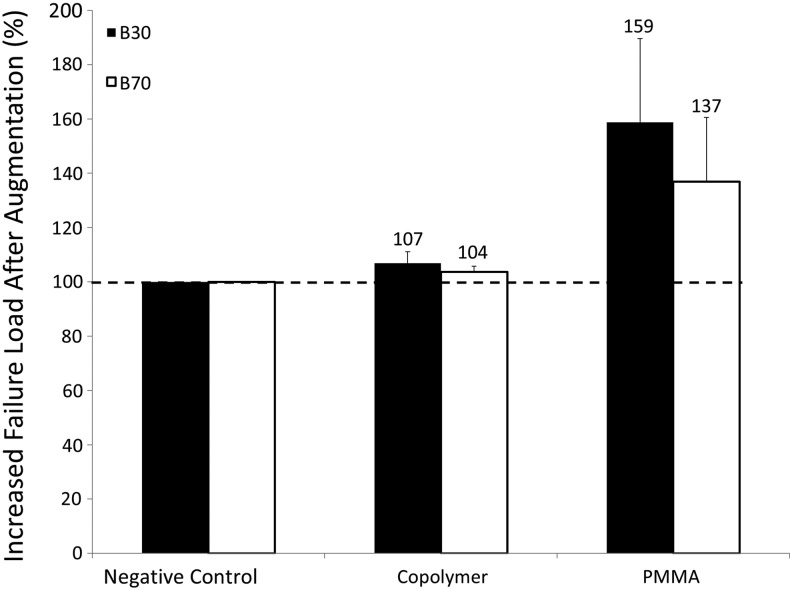
The spine is the most common site for secondary bone metastases, and clinical management for fractures is based on size and geometry of the defect. About 75% of the bone needs to be damaged before lesions are detectable, so clinical tools should measure changes in both geometry and material properties. We have developed an automated, user-friendly, Spine Cancer Assessment (SCA) image-based analysis method that builds on a platform designed for clinical practice providing failure characteristics of vertebrae. The objectives of this study were to (1) validate SCA predictions with experimental failure load outcomes; (2) evaluate the planning capabilities for prophylactic vertebroplasty procedures; and (3) investigate the effect of computed tomography (CT) protocols on predicted failure loads. Twenty-one vertebrae were randomly divided into two groups: (1) simulated defect without treatment (negative control) [n = 9] and (2) with treatment [n = 12]. Defects were created and a polymeric biomaterial was injected into the vertebrae in the treated-defect group. Spines were scanned, reconstructed with two algorithms, and analyzed for fracture loads. To virtually plan for prophylactic intervention, vertebrae with empty lesions were simulated to be augmented with either poly(methyl methacrylate) (PMMA) or a novel bone replacement copolymer, poly(propylene fumarate-co-caprolactone) [P(PF-co-CL)]. Axial rigidities were calculated from the CT images. Failure loads, determined from the cross section with the lowest axial rigidity, were compared with experimental values. Predicted loads correlated well with experimental outcomes (R(2) = 0.73, p < 0.0001). Predictions from negative control specimens highly correlated with measured values (R(2) = 0.90, p < 0.0001). Although a similar correlation was obtained using both algorithms, the smooth reconstruction (B30) tended to underestimate predicted failure loads by ∼50% compared with the ∼10% underestimate of the sharp reconstruction (B70). Percent increase in failure loads after virtual vertebroplasty showed a higher increase in samples with PMMA compared with those with copolymer. The SCA method developed in this study calculated failure loads from quantitative computed tomography scans in vertebrae with simulated metastatic lytic defects, with or without treatment, facilitating clinical applicability and providing more reliable guidelines for physicians to select appropriate treatment options. Furthermore, the analysis could accommodate augmentation planning procedures that aimed to determine the optimum material that would increase vertebral body failure load.
Figures



References
-
- American Cancer Society. Cancer Prevalence: How Many People Have Cancer? www.cancer.org, 2014
-
- American Academy of Orthopaedic Surgeons. Metastatic Bone Disease. http://orthoinfo.aaos.org
-
- Greenlee R.T., Hill-Harmon M.B., Murray T., and Thun M. Cancer statistics, 2001. CA Cancer J Clin 51, 15, 2001 - PubMed
-
- Wong D.A., Fornasier V.L., and MacNab I. Spinal metastases: the obvious, the occult, and the impostors. Spine (Phila Pa 1976) 15, 1, 1990 - PubMed
-
- Ahn H., Mousavi P., Roth S., Reidy D., Finkelstein J., and Whyne C. Stability of the metastatic spine pre and post vertebroplasty. J Spinal Disord Tech 19, 178, 2006 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
