

Diverting ileostomy during primary debulking surgery for ovarian cancer: Associated factors and postoperative outcomes
- PMID: 27261325
- PMCID: PMC4961543
- DOI: 10.1016/j.ygyno.2016.05.035
Diverting ileostomy during primary debulking surgery for ovarian cancer: Associated factors and postoperative outcomes
Abstract
Objective: To examine the use, as well as postoperative and long-term oncologic outcomes of diverting loop ileostomy (DI) during primary debulking surgery (PDS) for ovarian cancer.
Methods: Patients with stage II-IV ovarian, fallopian tube, or primary peritoneal carcinoma who underwent colon resection during PDS from 1/2005-1/2014 were identified. Demographic and clinical data were analyzed.
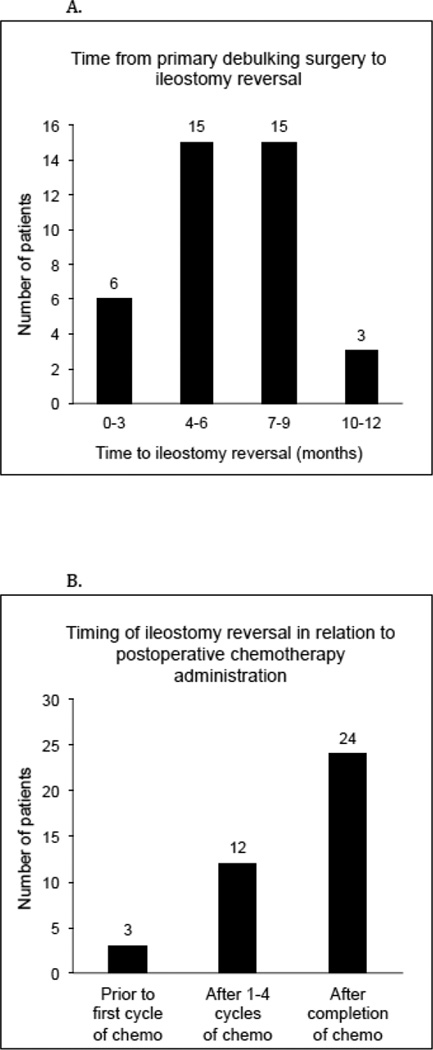
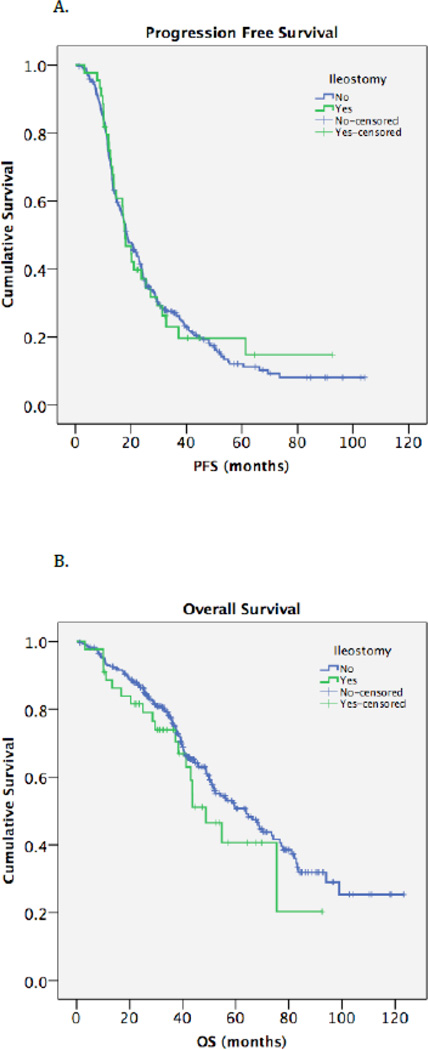
Results: Of 331 patients, 320 (97%) had stage III/IV disease and 278 (84%) had disease of high-grade serous histology. Forty-four (13%) underwent a DI. There were no significant differences in age, comorbidity index, smoking status, serum albumin, or attending surgeon between the DI and non-DI groups. Operative time (OR=1.21; 95% CI, 1.03-1.42; p=0.02) and length of rectosigmoid resection (OR=1.04; 95% CI, 1.01-1.08; p=0.02) were predictors of DI on multivariable analysis. The overall anastomotic leak rate was 6%. A comparison of groups (DI vs non-DI) showed no significant differences in major complications (30% vs 23%; p=0.41), anastomotic leak rate (5% vs 7%; p=0.60), hospital length of stay (10 vs 9days; p=0.25), readmission rate (23% vs 17%; p=0.33), or interval to postoperative chemotherapy (41 vs 40days; p=0.20), respectively. Ileostomy reversal was successful in 89% of patients. Median follow-up was 52.6months. There were no differences in median progression-free (17.9 vs 18.6months; p=0.88) and overall survival (48.7 vs 63.8months; p=0.25) between the groups.
Conclusions: In patients undergoing PDS, those with longer operative time and greater length of rectosigmoid resection more commonly underwent DI. DI does not appear to compromise postoperative outcomes or long-term survival.
Keywords: Anastomotic leak; Diverting ileostomy; Ovarian cancer; Postoperative outcomes; Primary debulking surgery; Rectosigmoid resection.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016 Jan;66(1):7–30. - PubMed
-
- Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol. 2002 Mar 1;20(5):1248–1259. - PubMed
-
- Phitayakorn R, Delaney CP, Reynolds HL, Champagne BJ, Heriot AG, Neary P, et al. Standardized algorithms for management of anastomotic leaks and related abdominal and pelvic abscesses after colorectal surgery. World J Surg. 2008 Jun;32(6):1147–1156. - PubMed
-
- Obermair A, Hagenauer S, Tamandl D, Clayton RD, Nicklin JL, Perrin LC, et al. Safety and efficacy of low anterior en bloc resection as part of cytoreductive surgery for patients with ovarian cancer. Gynecol Oncol. 2001 Oct;83(1):115–120. - PubMed
-
- Mourton SM, Temple LK, Abu-Rustum NR, Gemignani ML, Sonoda Y, Bochner BH, et al. Morbidity of rectosigmoid resection and primary anastomosis in patients undergoing primary cytoreductive surgery for advanced epithelial ovarian cancer. Gynecol Oncol. 2005 Dec;99(3):608–614. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
