

The Effects of the Transition From Medicaid to Medicare on Health Care Use for Adults With Mental Illness
- PMID: 27261640
- PMCID: PMC4982773
- DOI: 10.1097/MLR.0000000000000572
The Effects of the Transition From Medicaid to Medicare on Health Care Use for Adults With Mental Illness
Abstract
Background: The transition from Medicaid-only to dual Medicare/Medicaid coverage has the potential to reduce financial barriers to health care for patients with serious mental illness through increased coverage or expanded access to clinicians as their reimbursement increases.
Aims: To estimate the effect of dual coverage after Medicaid enrollment during the required waiting period among adults with serious mental illness on health care use, overall and related to mental health and substance use disorders (MHSUD).
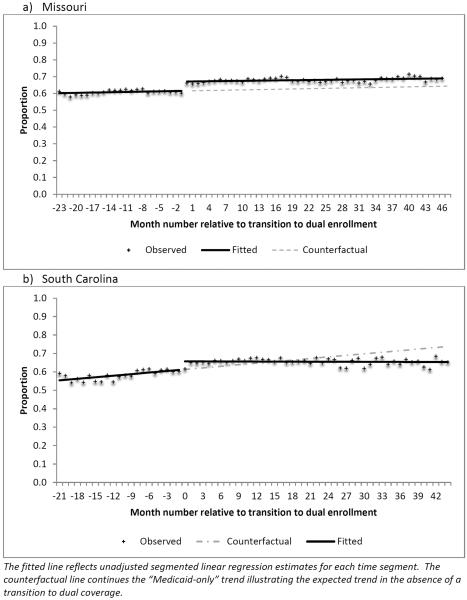
Methods: Data include enrollment and claims from Medicaid and Medicare in Missouri and South Carolina, from January 2004 to December 2007. We used an interrupted time-series design to estimate the effect of dual coverage on average use of outpatient, emergency department (ED), and inpatient care/month.
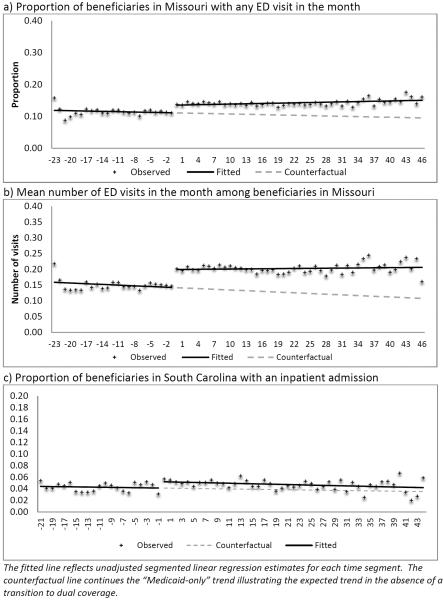
Results: After 12 months of dual coverage, the probability of outpatient care use increased in both states from 4% to 9%. In Missouri, the mean probability and frequency of ED visits, total and MHSUD related, increased by 21%-32%; the probability of all-cause and MHSUD-related inpatient admissions increased by 10% and 19%, respectively. In South Carolina, the mean probability of any inpatient admission increased by 27% and of any MHSUD-related inpatient admission by 42%.
Discussion: The increase in use of outpatient care is consistent with the expected increase in coverage of, and payment for, outpatient services under dual coverage relative to Medicaid-only. Sustained increases in ED and inpatient admissions raise questions regarding the complexity of obtaining care under 2 programs, pent-up demand among beneficiaries pretransition, and the complementarity of outpatient and inpatient service use.
Figures
References
-
- Rupp K, Davies P, Strand A. Disabiltiy Benefit Coverage and Program Interactions in the Working-Age Population. Social Security Bulletin. 2008;68:1–30. - PubMed
-
- Medicare Payment Advisory Commission . Report to Congress: Aligning Incentives in Medicare. Washington, D.C.: 2010. pp. 1–287.
-
- U.S. Government Accountability Office . Medicaid: A small share of enrollees consistently accounted for a large share of expenditures. Washington, D.C.: 2015. GAO-15-4604.
-
- Frank RG, Epstein AM. Factors Associated With High Levels Of Spending For Younger Dually Eligible Beneficiaries With Mental Disorders. Health Affairs. 2014;33:1006–1013. - PubMed
-
- Buck JA, Teich JL, Bae J, et al. Mental health and substance abuse services in ten state Medicaid programs. Administration and Policy in Mental Health. 2001;28:181–192. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
