

A prospective multicenter cohort study of frailty in younger critically ill patients
- PMID: 27263535
- PMCID: PMC4893838
- DOI: 10.1186/s13054-016-1338-x
A prospective multicenter cohort study of frailty in younger critically ill patients
Erratum in
-
Erratum to: A prospective multicenter cohort study of frailty in younger critically ill patients.Crit Care. 2016 Jul 19;20(1):223. doi: 10.1186/s13054-016-1393-3. Crit Care. 2016. PMID: 27435023 Free PMC article. No abstract available.
Abstract
Background: Frailty is a multidimensional syndrome characterized by loss of physiologic and cognitive reserve that heightens vulnerability. Frailty has been well described among elderly patients (i.e., 65 years of age or older), but few studies have evaluated frailty in nonelderly patients with critical illness. We aimed to describe the prevalence, correlates, and outcomes associated with frailty among younger critically ill patients.
Methods: We conducted a prospective cohort study of 197 consecutive critically ill patients aged 50-64.9 years admitted to intensive care units (ICUs) at six hospitals across Alberta, Canada. Frailty was defined as a score ≥5 on the Clinical Frailty Scale before hospitalization. Multivariable analyses were used to evaluate factors independently associated with frailty before ICU admission and the independent association between frailty and outcome.
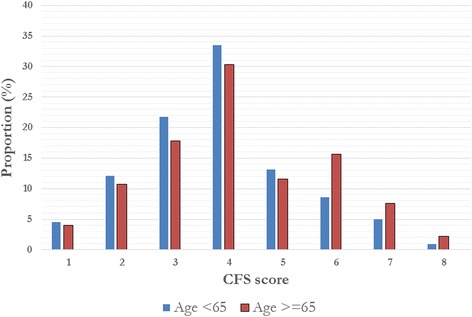
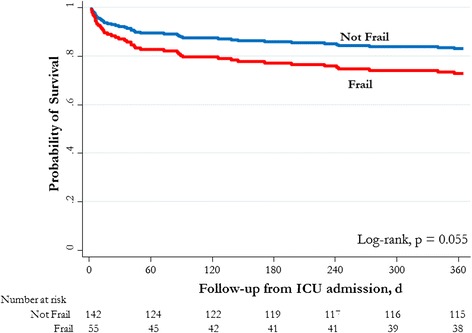
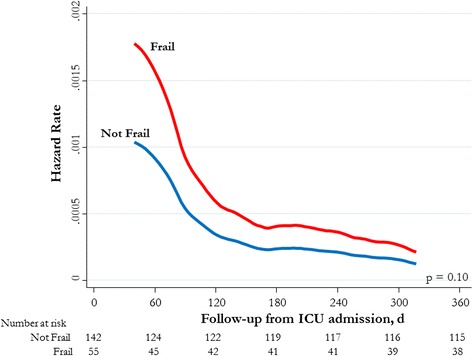
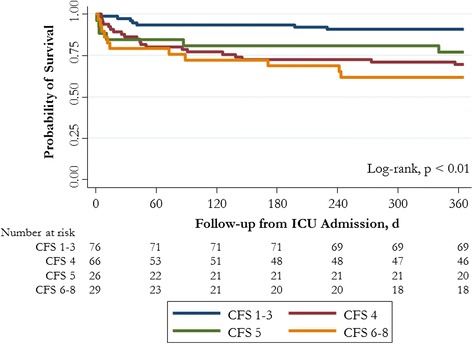
Results: In the 197 patients in the study, mean (SD) age was 58.5 (4.1) years, 37 % were female, 73 % had three or more comorbid illnesses, and 28 % (n = 55; 95 % CI 22-35) were frail. Factors independently associated with frailty included not being completely independent (adjusted OR [aOR] 4.4, 95 % CI 1.8-11.1), connective tissue disease (aOR 6.0, 95 % CI 2.1-17.0), and hospitalization within the preceding year (aOR 3.3, 95 % CI 1.3-8.1). There were no significant differences between frail and nonfrail patients in reason for admission, Acute Physiology and Chronic Health Evaluation II score, preference for life support, or treatment intensity. Younger frail patients did not have significantly longer (median [interquartile range]) hospital stay (26 [9-68] days vs. 19 [10-43] days; p = 0.4), but they had greater 1-year rehospitalization rates (61 % vs. 40 %; p = 0.02) and higher 1-year mortality (33 % vs. 20 %; adjusted HR 1.8, 95 % CI 1.0-3.3; p = 0.039).
Conclusions: Prehospital frailty is common among younger critically ill patients, and in this study it was associated with higher rates of mortality at 1 year and with rehospitalization. Our data suggest that frailty should be considered in younger adults admitted to the ICU, not just in the elderly. Additional research is needed to further characterize frailty in younger critically ill patients, along with the ideal instruments for identification.
Keywords: Critical illness; Frailty; Health services; Intensive care unit; Mortality; Quality of life.
Figures
Comment in
-
The younger frail critically ill patient: a newly recognised phenomenon in intensive care?Crit Care. 2016 Nov 1;20(1):349. doi: 10.1186/s13054-016-1526-8. Crit Care. 2016. PMID: 27799055 Free PMC article. No abstract available.
References
-
- Rockwood K, Howlett SE, MacKnight C, Beattie BL, Bergman H, Hebert R, et al. Prevalence, attributes, and outcomes of fitness and frailty in community-dwelling older adults: report from the Canadian Study of Health and Aging. J Gerontol A Biol Sci Med Sci. 2004;59(12):1310–7. doi: 10.1093/gerona/59.12.1310. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
