

Extending Aromatase-Inhibitor Adjuvant Therapy to 10 Years
- PMID: 27264120
- PMCID: PMC5024713
- DOI: 10.1056/NEJMoa1604700
Extending Aromatase-Inhibitor Adjuvant Therapy to 10 Years
Abstract
Background: Treatment with an aromatase inhibitor for 5 years as up-front monotherapy or after tamoxifen therapy is the treatment of choice for hormone-receptor-positive early breast cancer in postmenopausal women. Extending treatment with an aromatase inhibitor to 10 years may further reduce the risk of breast-cancer recurrence.
Methods: We conducted a double-blind, placebo-controlled trial to assess the effect of the extended use of letrozole for an additional 5 years. Our primary end point was disease-free survival.
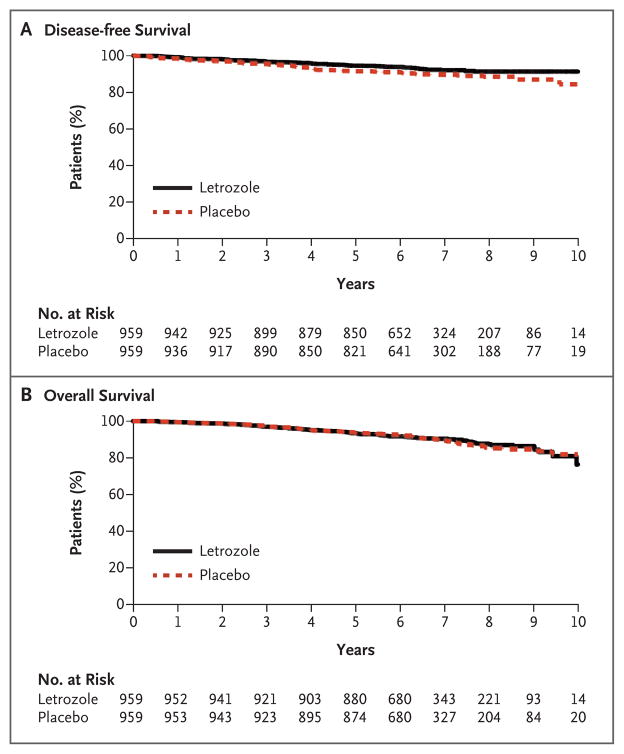
Results: We enrolled 1918 women. After a median follow-up of 6.3 years, there were 165 events involving disease recurrence or the occurrence of contralateral breast cancer (67 with letrozole and 98 with placebo) and 200 deaths (100 in each group). The 5-year disease-free survival rate was 95% (95% confidence interval [CI], 93 to 96) with letrozole and 91% (95% CI; 89 to 93) with placebo (hazard ratio for disease recurrence or the occurrence of contralateral breast cancer, 0.66; P=0.01 by a two-sided log-rank test stratified according to nodal status, prior adjuvant chemotherapy, the interval from the last dose of aromatase-inhibitor therapy, and the duration of treatment with tamoxifen). The rate of 5-year overall survival was 93% (95% CI, 92 to 95) with letrozole and 94% (95% CI, 92 to 95) with placebo (hazard ratio, 0.97; P=0.83). The annual incidence rate of contralateral breast cancer in the letrozole group was 0.21% (95% CI, 0.10 to 0.32), and the rate in the placebo group was 0.49% (95% CI, 0.32 to 0.67) (hazard ratio, 0.42; P=0.007). Bone-related toxic effects occurred more frequently among patients receiving letrozole than among those receiving placebo, including a higher incidence of bone pain, bone fractures, and new-onset osteoporosis. No significant differences between letrozole and placebo were observed in scores on most subscales measuring quality of life.
Conclusions: The extension of treatment with an adjuvant aromatase inhibitor to 10 years resulted in significantly higher rates of disease-free survival and a lower incidence of contralateral breast cancer than those with placebo, but the rate of overall survival was not higher with the aromatase inhibitor than with placebo. (Funded by the Canadian Cancer Society and others; ClinicalTrials.gov numbers, NCT00003140 and NCT00754845.).
Figures

Comment in
-
Changing Adjuvant Breast-Cancer Therapy with a Signal for Prevention.N Engl J Med. 2016 Jul 21;375(3):274-5. doi: 10.1056/NEJMe1606031. Epub 2016 Jun 5. N Engl J Med. 2016. PMID: 27263869 No abstract available.
-
Extra five years of aromatase inhibitors increases disease-free survival in breast cancer.BMJ. 2016 Jun 5;353:i3153. doi: 10.1136/bmj.i3153. BMJ. 2016. PMID: 27268511 No abstract available.
-
Extending Adjuvant Aromatase-Inhibitor Therapy to 10 Years.N Engl J Med. 2016 Oct 20;375(16):1591. doi: 10.1056/NEJMc1610719. N Engl J Med. 2016. PMID: 27797308 No abstract available.
-
Extending Adjuvant Aromatase-Inhibitor Therapy to 10 Years.N Engl J Med. 2016 Oct 20;375(16):1590. doi: 10.1056/NEJMc1610719. N Engl J Med. 2016. PMID: 27797309 No abstract available.
-
Extending Adjuvant Aromatase-Inhibitor Therapy to 10 Years.N Engl J Med. 2016 Oct 20;375(16):1590-1. doi: 10.1056/NEJMc1610719. N Engl J Med. 2016. PMID: 28102998 No abstract available.
References
-
- Early Breast Cancer Trialists’ Collaborative Group. Tamoxifen for early breast cancer. Cochrane Database Syst Rev. 2001;1:CD000486. - PubMed
-
- Gray RG, Rea D, Handling K, et al. aTTom (adjuvant Tamoxifen–To offer more?): randomized trial of 10 versus 5 years of adjuvant tamoxifen among 6,934 women with estrogen receptor-positive (ER+) or ER untested breast cancer — preliminary results. J Clin Oncol. 2008;26(Suppl 10s):513. abstract.
-
- Strasser-Weippl K, Badovinac-Crnjevic T, Fan L, Goss PE. Extended adjuvant endocrine therapy in hormone-receptor positive breast cancer. Breast. 2013;22(Suppl 2):S171–5. - PubMed
-
- Tu D. Minimization procedure. In: Chow SC, editor. Encyclopedia of biopharmaceutical statistics. 2. New York: Marcel Dekker; 2003. pp. 614–8.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- CA37981/CA/NCI NIH HHS/United States
- U10 CA037981/CA/NCI NIH HHS/United States
- UG1 CA189805/CA/NCI NIH HHS/United States
- CA180863/CA/NCI NIH HHS/United States
- CA189953/CA/NCI NIH HHS/United States
- CA189805/CA/NCI NIH HHS/United States
- U10 CA180828/CA/NCI NIH HHS/United States
- CA180888/CA/NCI NIH HHS/United States
- U10 CA180838/CA/NCI NIH HHS/United States
- U10 CA067753/CA/NCI NIH HHS/United States
- CA16116/CA/NCI NIH HHS/United States
- U10 CA180802/CA/NCI NIH HHS/United States
- N01 CA013612/CA/NCI NIH HHS/United States
- U10 CA077202/CA/NCI NIH HHS/United States
- CA077202/CA/NCI NIH HHS/United States
- U10 CA021115/CA/NCI NIH HHS/United States
- U10 CA013612/CA/NCI NIH HHS/United States
- CA180820/CA/NCI NIH HHS/United States
- CA180802/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- U10 CA180791/CA/NCI NIH HHS/United States
- U10 CA180863/CA/NCI NIH HHS/United States
- U10 CA016116/CA/NCI NIH HHS/United States
- CA67753/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- CA21115/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- UG1 CA189953/CA/NCI NIH HHS/United States
- CA180828/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical