

Maternal influenza and birth outcomes: systematic review of comparative studies
- PMID: 27264387
- PMCID: PMC5216449
- DOI: 10.1111/1471-0528.14143
Maternal influenza and birth outcomes: systematic review of comparative studies
Abstract
Background: Although pregnant women are considered at high risk for severe influenza disease, comparative studies of maternal influenza and birth outcomes have not been comprehensively summarised.
Objective: To review comparative studies evaluating maternal influenza disease and birth outcomes.
Search strategy: We searched bibliographic databases from inception to December 2014.
Selection criteria: Studies of preterm birth, small-for-gestational-age (SGA) birth or fetal death, comparing women with and without clinical influenza illness or laboratory-confirmed influenza infection during pregnancy.
Data collection and analysis: Two reviewers independently abstracted data and assessed study quality.
Main results: Heterogeneity across 16 studies reporting preterm birth precluded meta-analysis. In a subgroup of the highest-quality studies, two reported significantly increased preterm birth (risk ratios (RR) from 2.4 to 4.0) following severe 2009 pandemic H1N1 (pH1N1) influenza illness, whereas those assessing mild-to-moderate pH1N1 or seasonal influenza found no association. Five studies of SGA birth showed no discernible patterns with respect to influenza disease severity (pooled odds ratio 1.24; 95% CI 0.96-1.59). Two fetal death studies were of sufficient quality and size to permit meaningful interpretation. Both reported an increased risk of fetal death following maternal pH1N1 disease (RR 1.9 for mild-to-moderate disease and 4.2 for severe disease).
Conclusions: Comparative studies of preterm birth, SGA birth and fetal death following maternal influenza disease are limited in number and quality. An association between severe pH1N1 disease and preterm birth and fetal death was reported by several studies; however, these limited data do not permit firm conclusions on the magnitude of any association.
Tweetable abstract: Comparative studies are limited in quality but suggest severe pandemic H1N1 influenza increases preterm birth.
Keywords: Fetal death; influenza; pregnancy; preterm birth; small-for-gestational-age birth; systematic review.
© 2016 World Health Organization; licensed by John Wiley & Sons Ltd on behalf of Royal College of Obstetricians and Gynaecologists.
Figures


 ’ indicates a Newcastle‐Ottawa Score ≥8, risk of diagnostic ascertainment bias not rated as ‘very high’, and exposure not measured using self‐reported questionnaire. cCrude estimates were used in place of adjusted estimates when the latter were not provided. dHansen (2012)40 is shown twice: one estimate for 2009 A (
’ indicates a Newcastle‐Ottawa Score ≥8, risk of diagnostic ascertainment bias not rated as ‘very high’, and exposure not measured using self‐reported questionnaire. cCrude estimates were used in place of adjusted estimates when the latter were not provided. dHansen (2012)40 is shown twice: one estimate for 2009 A (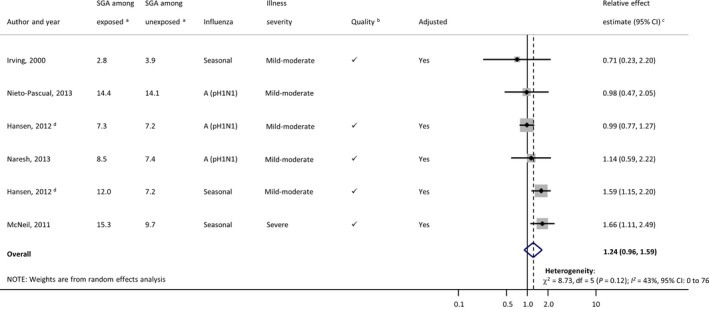
 ’ indicates a Newcastle‐Ottawa Score ≥8, risk of diagnostic ascertainment bias not rated as ‘very high’, and exposure not measured using self‐reported questionnaire. cCrude estimates were used in place of adjusted estimates when the latter were not provided. dHansen (2012)40 is shown twice: one estimate for 2009 A (
’ indicates a Newcastle‐Ottawa Score ≥8, risk of diagnostic ascertainment bias not rated as ‘very high’, and exposure not measured using self‐reported questionnaire. cCrude estimates were used in place of adjusted estimates when the latter were not provided. dHansen (2012)40 is shown twice: one estimate for 2009 A (
 ’ indicates a Newcastle‐Ottawa Score ≥8, risk of diagnostic ascertainment bias not rated as ‘very high’, and exposure not measured using self‐reported questionnaire. C Crude estimates were used in place of adjusted estimates when the latter were not provided. dNieto‐Pascual (2013)37 is shown twice: one estimate for abortion (
’ indicates a Newcastle‐Ottawa Score ≥8, risk of diagnostic ascertainment bias not rated as ‘very high’, and exposure not measured using self‐reported questionnaire. C Crude estimates were used in place of adjusted estimates when the latter were not provided. dNieto‐Pascual (2013)37 is shown twice: one estimate for abortion (Comment in
-
Outcomes of flu in pregnancy: summarizing what is known.BJOG. 2017 Jan;124(1):60. doi: 10.1111/1471-0528.14174. Epub 2016 Jun 20. BJOG. 2017. PMID: 27319743 No abstract available.
References
-
- Harris J. Influenza occurring in pregnant women. J Am Med Assoc 1919;72:978–80.
-
- Freeman DW, Barno A. Deaths from Asian influenza associated with pregnancy. Am J Obstet Gynecol 1959;78:1172–5. - PubMed
-
- Neuzil KM, Reed GW, Mitchel EF, Simonsen L, Griffin MR. Impact of influenza on acute cardiopulmonary hospitalizations in pregnant women. Am J Epidemiol 1998;148:1094–102. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
