

Simultaneous anterior and posterior serosal mapping of gastric slow-wave dysrhythmias induced by vasopressin
- PMID: 27265885
- PMCID: PMC5140776
- DOI: 10.1113/EP085697
Simultaneous anterior and posterior serosal mapping of gastric slow-wave dysrhythmias induced by vasopressin
Abstract
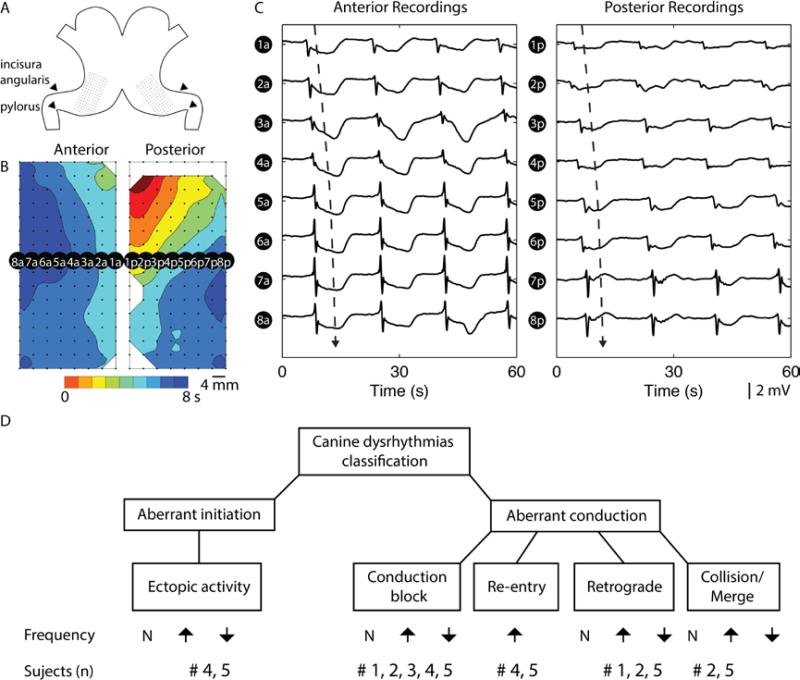
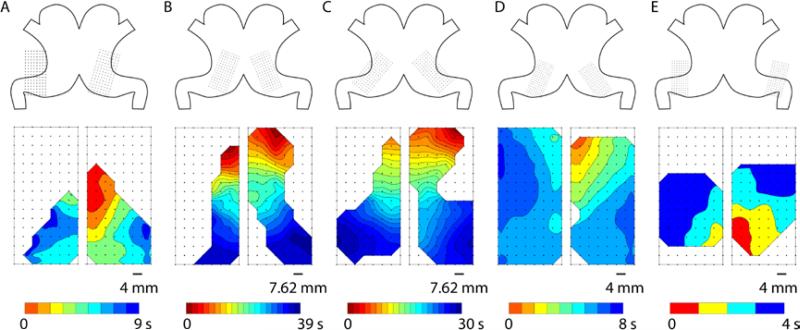
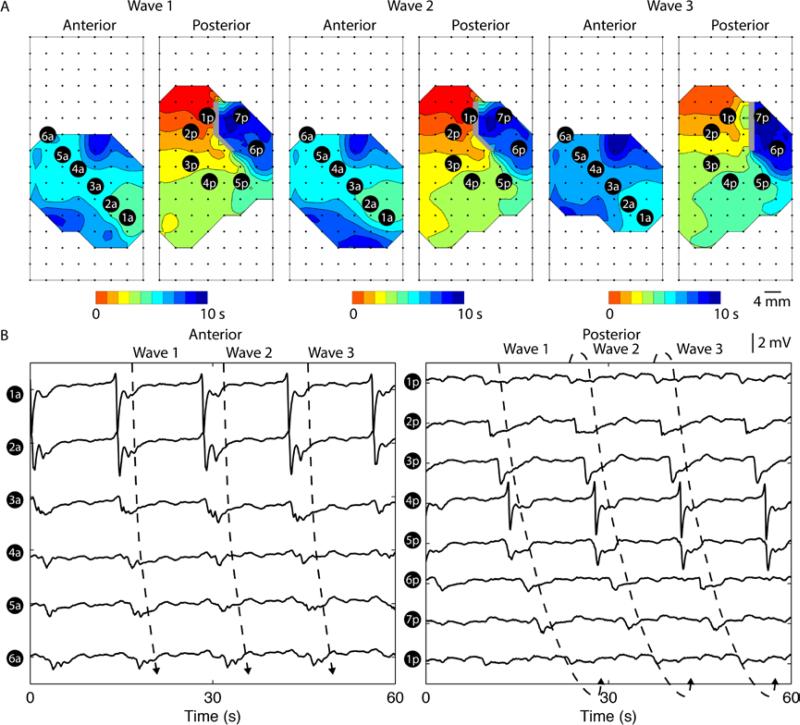
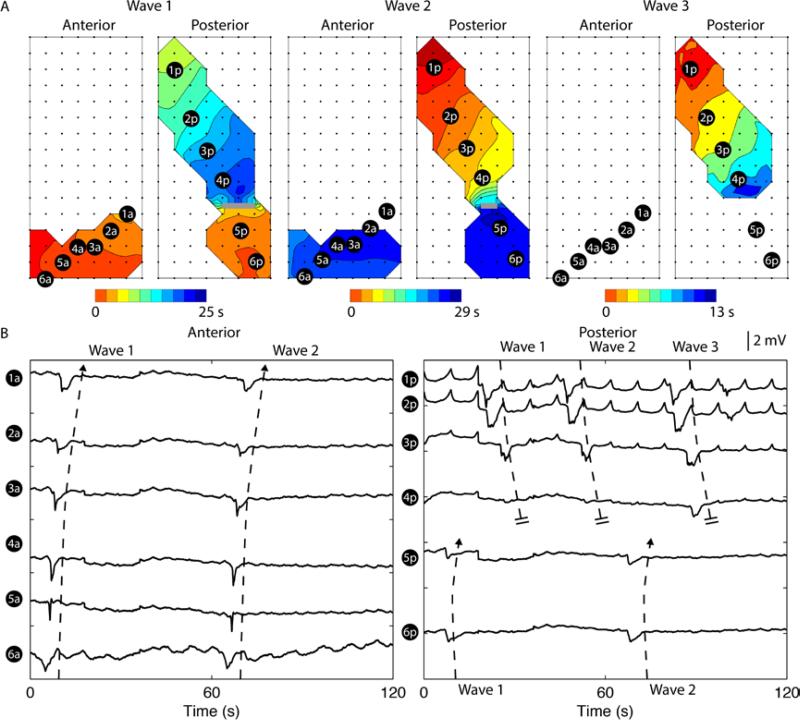
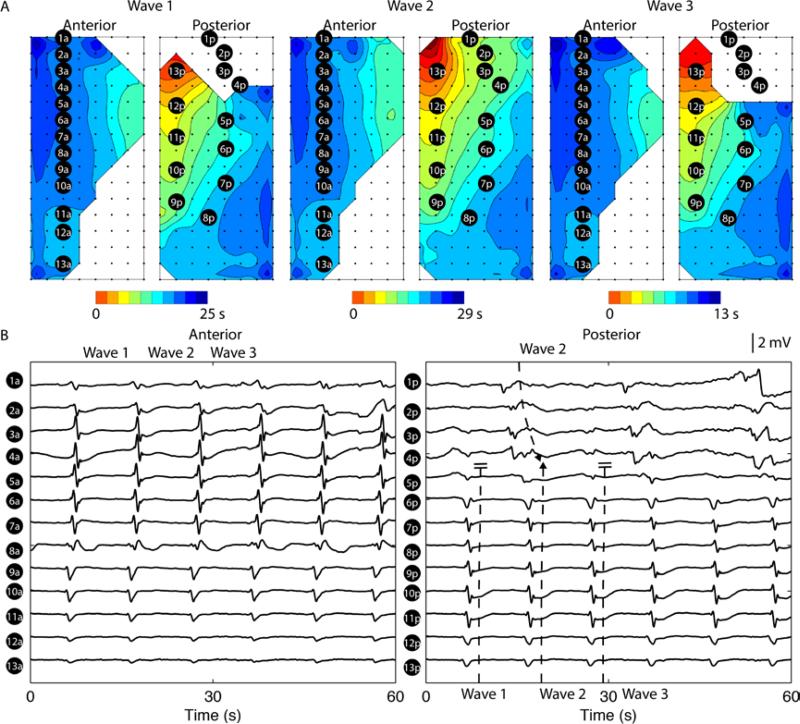
What is the central question of this study? This study aimed to provide the first comparison of simultaneous high-resolution mapping of anterior and posterior gastric serosa over sustained periods. What is the main finding and its importance? Episodes of spontaneous gastric slow-wave dysrhythmias increased significantly following intravenous infusion of vasopressin compared with the baseline state. A number of persistent dysrhythmias were defined, including ectopic activation, conduction block, rotor, retrograde and collision/merger of wavefronts. Slow-wave dysrhythmias could occur either simultaneously or independently on the anterior and posterior gastric serosa, and interacted depending on activation-repolarization and frequency dynamics. High-resolution mapping enables mechanistic insights into gastric slow-wave dysrhythmias and is now achieving clinical translation. However, previous studies have focused mainly on dysrhythmias occurring on the anterior gastric wall. The present study simultaneously mapped the anterior and posterior gastric serosa during episodes of dysrhythmias induced by vasopressin to aid understanding of dysrhythmia initiation, maintenance and termination. High-resolution mapping (8 × 16 electrodes on each serosa; 20-74 cm2 ) was performed in anaesthetized dogs. Baseline recordings (21 ± 8 min) were followed by intravenous infusion of vasopressin (0.1-0.5 IU ml-1 at 60-190 ml h-1 ) and further recordings (22 ± 13 min). Slow-wave activation maps, amplitudes, velocity, interval and frequency were calculated, and differences compared between baseline and postinfusion. All dogs demonstrated an increased prevalence of dysrhythmic events following infusion of vasopressin (17 versus 51%). Both amplitude and velocity demonstrated significant differences (baseline versus postinfusion: 3.6 versus 2.2 mV; 7.7 versus 6.5 mm s-1 ; P < 0.05 for both). Dysrhythmias occurred simultaneously or independently on the anterior and posterior serosa, and then interacted according to frequency dynamics. A number of persistent dysrhythmias were compared, including the following: ectopic activation (n = 2 animals), conduction block (n = 1), rotor (n = 2), retrograde (n = 3) and collision/merger of wavefronts (n = 2). We conclude that infusion of vasopressin induces gastric dysrhythmias, which occur across a heterogeneous range of frequencies and patterns. The results demonstrate that different classes of gastric dysrhythmias may arise simultaneously or independently in one or both surfaces of the serosa, then interact according to their relative frequencies. These results will help to inform interpretation of clinical dysrhythmia.
Keywords: gastric dysrhythmias; gastric electrical activity; high-resolution mapping; interstitial cells of Cajal.
© 2016 The Authors. Experimental Physiology © 2016 The Physiological Society.
Figures
Comment in
-
The 'dark' side of the stomach.Exp Physiol. 2017 Jan 1;102(1):134. doi: 10.1113/EP086036. Exp Physiol. 2017. PMID: 28044403 No abstract available.
-
Reply.Exp Physiol. 2017 Jan 1;102(1):135. doi: 10.1113/EP086141. Exp Physiol. 2017. PMID: 28044406 No abstract available.
References
-
- Abell TL, Malagelada JR. Glucagon-evoked gastric dysrhythmias in humans shown by an improved electrogastrographic technique. Gastroenterology. 1985;88:1932–1940. - PubMed
-
- Angeli TR, Cheng LK, Du P, Wang TH-H, Bernard CE, Vannucchi M-G, Faussone-Pellegrini MS, Lahr C, Vather R, Windsor JA, Farrugia G, Abell TL, O'Grady G. Loss of Interstitial Cells of Cajal and Patterns of Gastric Dysrhythmia in Patients With Chronic Unexplained Nausea and Vomiting. Gastroenterology. 2015;149:56–66. e5. - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources