

Identifying improvements to complex pathways: evidence synthesis and stakeholder engagement in infant congenital heart disease
- PMID: 27266768
- PMCID: PMC4908909
- DOI: 10.1136/bmjopen-2015-010363
Identifying improvements to complex pathways: evidence synthesis and stakeholder engagement in infant congenital heart disease
Abstract
Objectives: Many infants die in the year following discharge from hospital after surgical or catheter intervention for congenital heart disease (3-5% of discharged infants). There is considerable variability in the provision of care and support in this period, and some families experience barriers to care. We aimed to identify ways to improve discharge and postdischarge care for this patient group.
Design: A systematic evidence synthesis aligned with a process of eliciting the perspectives of families and professionals from community, primary, secondary and tertiary care.
Setting: UK.
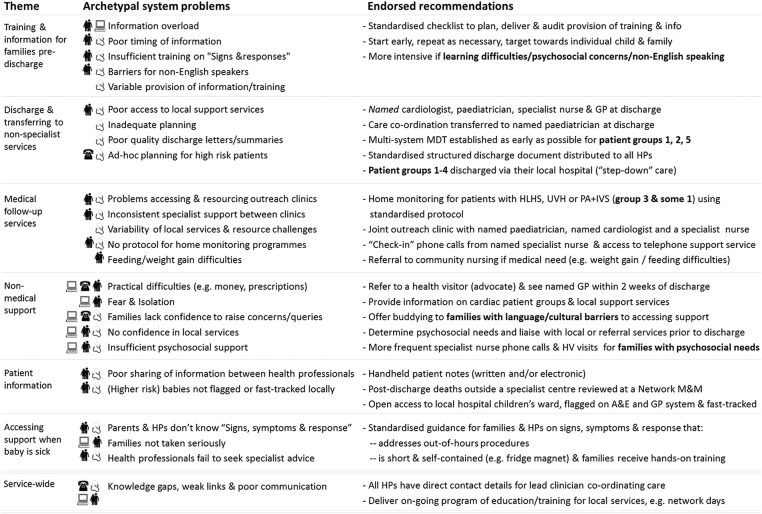
Results: A set of evidence-informed recommendations for improving the discharge and postdischarge care of infants following intervention for congenital heart disease was produced. These address known challenges with current care processes and, recognising current resource constraints, are targeted at patient groups based on the number of patients affected and the level and nature of their risk of adverse 1-year outcome. The recommendations include: structured discharge documentation, discharging certain high-risk patients via their local hospital, enhanced surveillance for patients with certain (high-risk) cardiac diagnoses and an early warning tool for parents and community health professionals.
Conclusions: Our recommendations set out a comprehensive, system-wide approach for improving discharge and postdischarge services. This approach could be used to address challenges in delivering care for other patient populations that can fall through gaps between sectors and organisations.
Keywords: STATISTICS & RESEARCH METHODS.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
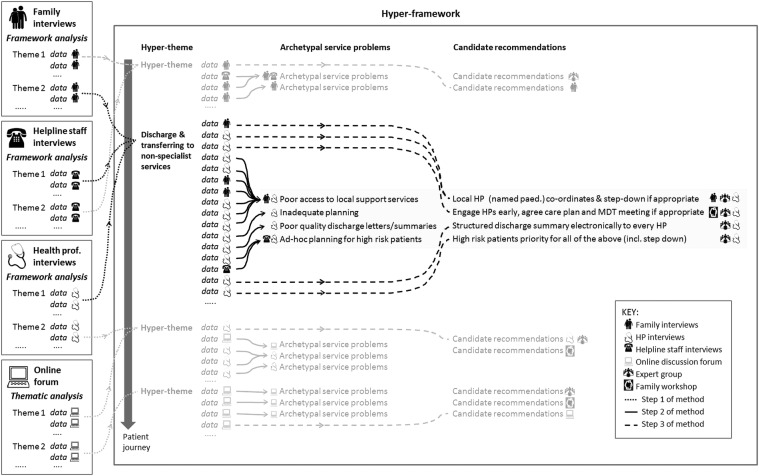
 ,
health professional interviews
,
health professional interviews  ,
helpline staff interviews
,
helpline staff interviews  and an online discussion forum
and an online discussion forum  . A&E, accident and emergency department; GP, general practitioner; HLHS, hypoplastic left heart syndrome; HP, health professional; IVS, intact ventricular septum; MDT, multidisciplinary team; M&M, mortality and morbidity meeting; PA, pulmonary atresia; UVH, functionally univentricular heart.
. A&E, accident and emergency department; GP, general practitioner; HLHS, hypoplastic left heart syndrome; HP, health professional; IVS, intact ventricular septum; MDT, multidisciplinary team; M&M, mortality and morbidity meeting; PA, pulmonary atresia; UVH, functionally univentricular heart.Similar articles
-
Parents' Experiences of Caring for Their Child at the Time of Discharge After Cardiac Surgery and During the Postdischarge Period: Qualitative Study Using an Online Forum.J Med Internet Res. 2018 May 9;20(5):e155. doi: 10.2196/jmir.9104. J Med Internet Res. 2018. PMID: 29743157 Free PMC article.
-
Going home after infant cardiac surgery: a UK qualitative study.Arch Dis Child. 2016 Apr;101(4):320-5. doi: 10.1136/archdischild-2015-308827. Epub 2016 Jan 29. Arch Dis Child. 2016. PMID: 26826171 Free PMC article.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Infant deaths in the UK community following successful cardiac surgery: building the evidence base for optimal surveillance, a mixed-methods study.Southampton (UK): NIHR Journals Library; 2016 May. Southampton (UK): NIHR Journals Library; 2016 May. PMID: 27252995 Free Books & Documents. Review.
-
Lessons for the UK on implementation and evaluation of breastfeeding support: evidence syntheses and stakeholder engagement.Health Soc Care Deliv Res. 2024 Jul;12(20):1-206. doi: 10.3310/DGTP5702. Health Soc Care Deliv Res. 2024. PMID: 39054917
Cited by
-
Evaluation of healthcare professionals' experiences of taking telephone calls from parents of children with congenital heart disease. A risky business.J Child Health Care. 2025 Jun;29(2):486-500. doi: 10.1177/13674935231222943. Epub 2024 Jan 4. J Child Health Care. 2025. PMID: 38174717 Free PMC article.
-
Learning to See: Using Mixed OR Methods to Model Radiology Staff Workload and Support Decision Making in CT.SN Comput Sci. 2022;3(5):361. doi: 10.1007/s42979-022-01244-4. Epub 2022 Jul 5. SN Comput Sci. 2022. PMID: 35818394 Free PMC article.
-
Improving the production of applied health research findings: insights from a qualitative study of operational research.Implement Sci. 2017 Sep 8;12(1):112. doi: 10.1186/s13012-017-0643-3. Implement Sci. 2017. PMID: 28886709 Free PMC article.
-
Combining qualitative and quantitative operational research methods to inform quality improvement in pathways that span multiple settings.BMJ Qual Saf. 2017 Aug;26(8):641-652. doi: 10.1136/bmjqs-2016-005636. Epub 2017 Jan 6. BMJ Qual Saf. 2017. PMID: 28062603 Free PMC article.
-
Parents' Experiences of Caring for Their Child at the Time of Discharge After Cardiac Surgery and During the Postdischarge Period: Qualitative Study Using an Online Forum.J Med Internet Res. 2018 May 9;20(5):e155. doi: 10.2196/jmir.9104. J Med Internet Res. 2018. PMID: 29743157 Free PMC article.
References
-
- NHS. Safe and sustainable: children's congenital cardiac services. NHS Specialist Services, 2011. http://www.specialisedservices.nhs.uk/safe_sustainable/childrens-congeni... (accessed 26 Feb 2011).
-
- NHS England. New congenital heart disease review. http://www.england.nhs.uk/ourwork/qual-clin-lead/chd/ (accessed 22 Jul 2015).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical