

Multimorbidity and use of hypnotic and anxiolytic drugs: cross-sectional and follow-up study in primary healthcare in Iceland
- PMID: 27267943
- PMCID: PMC4896036
- DOI: 10.1186/s12875-016-0469-0
Multimorbidity and use of hypnotic and anxiolytic drugs: cross-sectional and follow-up study in primary healthcare in Iceland
Abstract
Background: The prevalence of multimorbidity is increasing worldwide, presumably leading to an increased use of medicines. During the last decades the use of hypnotic and anxiolytic benzodiazepine derivatives and related drugs has increased dramatically. These drugs are frequently prescribed for people with a sleep disorder often merely designated as "insomnia" in the medical records and lacking a clear connection with the roots of the patients' problems. Our aim was to analyse the prevalence of multimorbidity in primary healthcare in Iceland, while concurrently investigating a possible association with the prevalence and incidence of hypnotic/anxiolytic prescriptions, short-term versus chronic use.
Methods: Data were retrieved from a comprehensive database of medical records from primary healthcare in Iceland to find multimorbid patients and prescriptions for hypnotics and anxiolytics, linking diagnoses (ICD-10) and prescriptions (2009-2012) to examine a possible association. Nearly 222,000 patients, 83 % being local residents in the capital area, who contacted 16 healthcare centres served in total by 140 general practitioners, were set as a reference to find the prevalence of multimorbidity as well as the prevalence and incidence of hypnotic/anxiolytic prescriptions.
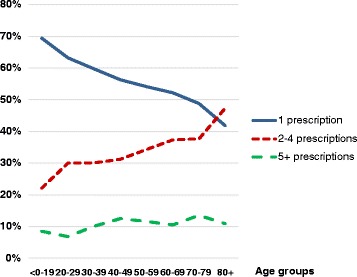
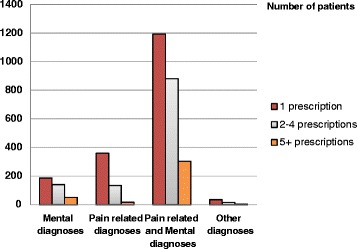
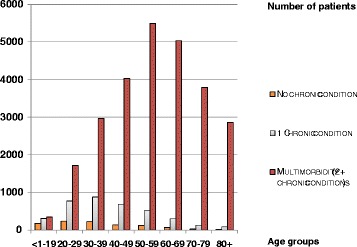
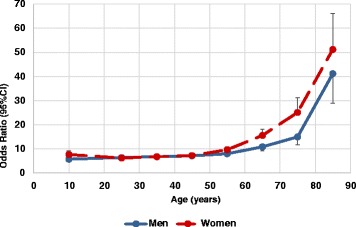
Results: The prevalence of multimorbidity in the primary care population was 35 %, lowest in the young, increasing with age up to the 80+ group where it dropped somewhat. The prevalence of hypnotic/anxiolytic prescriptions was 13.9 %. The incidence rate was 19.4 per 1000 persons per year in 2011, and 85 % of the patients prescribed hypnotics/anxiolytics were multimorbid. Compared to patients without multimorbidity, multimorbid patients were far more likely to be prescribed a hypnotic and/or an anxiolytic, OR = 14.9 (95 % CI = 14.4-15.4).
Conclusions: Patients with multiple chronic conditions are common in the primary care setting, and prevalence and incidence of hypnotic/anxiolytic prescriptions are high. Solely explaining use of these drugs by linear thinking, i.e. that "insomnia" leads to their prescription is probably simplistic, since the majority of patients prescribed these drugs are multimorbid having several chronic conditions which could lead to sleeping problems. However, multimorbidity as such is not an indication for hypnotics, and doctors should be urged to greater caution in their prescribing, bearing in mind non-pharmacological therapy options.
Keywords: Anxiolytics; Chronic health problems; Hypnotics; ICD-10; Insomnia; Multimorbidity; Multiple chronic conditions; Primary care.
Figures
Similar articles
-
[Antidepressants, anxiolytics and hypnotics prescribed to young adults before and after an economic crisis in Iceland - A cross-sectional study at the Primary Health Care of Reykjavik capital area].Laeknabladid. 2019 Oktober;105(10):427-432. doi: 10.17992/lbl.2019.10.250. Laeknabladid. 2019. PMID: 31571605 Icelandic.
-
Association between prescription of hypnotics/anxiolytics and mortality in multimorbid and non-multimorbid patients: a longitudinal cohort study in primary care.BMJ Open. 2019 Dec 5;9(12):e033545. doi: 10.1136/bmjopen-2019-033545. BMJ Open. 2019. PMID: 31811011 Free PMC article.
-
'Hypnotic' prescription patterns in a large managed-care population.Sleep Med. 2004 Sep;5(5):463-6. doi: 10.1016/j.sleep.2004.03.007. Sleep Med. 2004. PMID: 15341891
-
[Epidemiology of the use of anxiolytic and hypnotic drugs in France and in the world].Encephale. 1996 May-Jun;22(3):187-96. Encephale. 1996. PMID: 8767047 Review. French.
-
[Excessive prescribing of hypnotic and anxiolytic drugs in Japan].Nihon Rinsho. 2015 Jun;73(6):1049-56. Nihon Rinsho. 2015. PMID: 26065141 Review. Japanese.
Cited by
-
Medical Psychotropics in Forensic Autopsies in European Countries: Results from a Three-Year Retrospective Study in Spain.Toxics. 2022 Feb 1;10(2):64. doi: 10.3390/toxics10020064. Toxics. 2022. PMID: 35202250 Free PMC article.
-
Prevalence of insomnia and hypnotic use in Norwegian patients visiting their general practitioner.Fam Pract. 2023 Mar 28;40(2):352-359. doi: 10.1093/fampra/cmac103. Fam Pract. 2023. PMID: 36124938 Free PMC article.
-
Course of activities of daily living in nursing home residents with dementia from admission to 36-month follow-up.BMC Geriatr. 2020 Nov 20;20(1):488. doi: 10.1186/s12877-020-01877-1. BMC Geriatr. 2020. PMID: 33218298 Free PMC article.
-
Physical multimorbidity and subjective cognitive complaints among adults in the United Kingdom: a cross-sectional community-based study.Sci Rep. 2019 Aug 27;9(1):12417. doi: 10.1038/s41598-019-48894-8. Sci Rep. 2019. PMID: 31455875 Free PMC article.
-
Prescribing Analgesics to Older People: A Challenge for GPs.Int J Environ Res Public Health. 2020 Jun 5;17(11):4017. doi: 10.3390/ijerph17114017. Int J Environ Res Public Health. 2020. PMID: 32516932 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
