

Sequential administration of nivolumab and ipilimumab with a planned switch in patients with advanced melanoma (CheckMate 064): an open-label, randomised, phase 2 trial
- PMID: 27269740
- PMCID: PMC5474305
- DOI: 10.1016/S1470-2045(16)30126-7
Sequential administration of nivolumab and ipilimumab with a planned switch in patients with advanced melanoma (CheckMate 064): an open-label, randomised, phase 2 trial
Erratum in
-
Correction to Lancet Oncol 2016; 17: 953.Lancet Oncol. 2016 Jul;17(7):e270. doi: 10.1016/S1470-2045(16)30246-7. Epub 2016 Jun 28. Lancet Oncol. 2016. PMID: 27733291 No abstract available.
Abstract
Background: Concurrent administration of the immune checkpoint inhibitors nivolumab and ipilimumab has shown greater efficacy than either agent alone in patients with advanced melanoma, albeit with more high-grade adverse events. We assessed whether sequential administration of nivolumab followed by ipilimumab, or the reverse sequence, could improve safety without compromising efficacy.
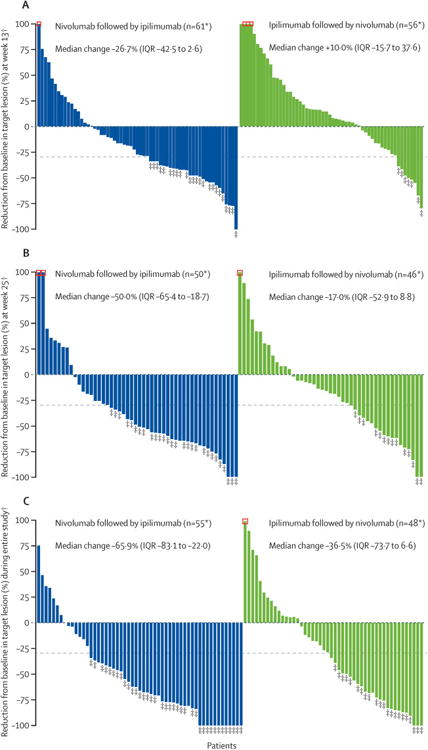
Methods: We did this randomised, open-label, phase 2 study at nine academic medical centres in the USA. Eligible patients (aged ≥18 years) with unresectable stage III or IV melanoma (treatment-naive or who had progressed after no more than one previous systemic therapy, with an Eastern Cooperative Oncology Group performance status of 0 or 1) were randomly assigned (1:1) to induction with intravenous nivolumab 3 mg/kg every 2 weeks for six doses followed by a planned switch to intravenous ipilimumab 3 mg/kg every 3 weeks for four doses, or the reverse sequence. Randomisation was done by an independent interactive voice response system with a permuted block schedule (block size four) without stratification factors. After induction, both groups received intravenous nivolumab 3 mg/kg every 2 weeks until progression or unacceptable toxicity. The primary endpoint was treatment-related grade 3-5 adverse events until the end of the induction period (week 25), analysed in the as-treated population. Secondary endpoints were the proportion of patients who achieved a response at week 25 and disease progression at weeks 13 and 25. Overall survival was a prespecified exploratory endpoint. This study is registered with ClinicalTrials.gov, number NCT01783938, and is ongoing but no longer enrolling patients.
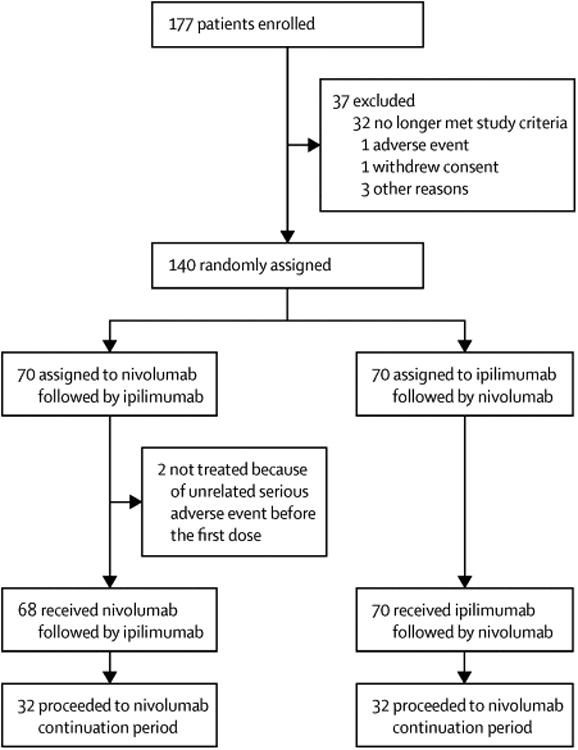
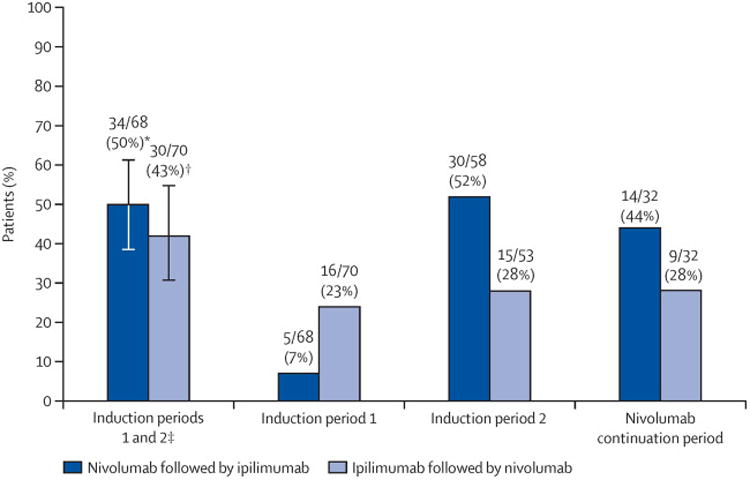
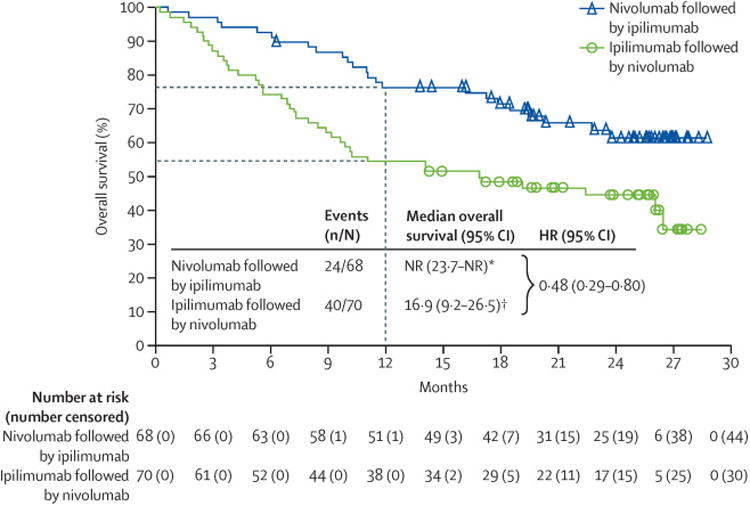
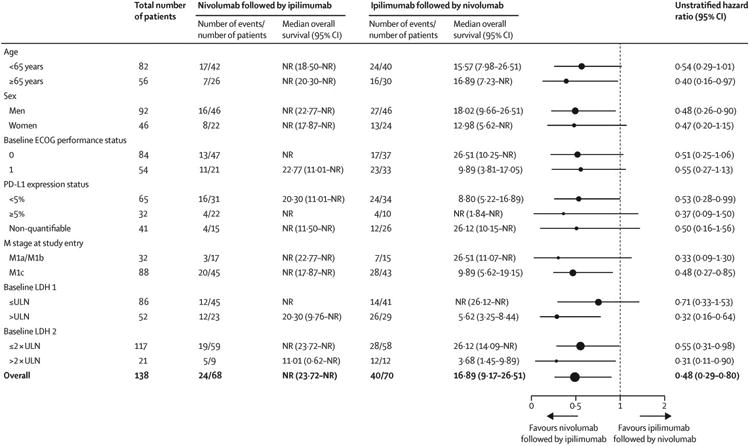
Findings: Between April 30, 2013, and July 21, 2014, 140 patients were enrolled and randomly assigned to nivolumab followed by ipilimumab (n=70) or to the reverse sequence of ipilimumab followed by nivolumab (n=70), of whom 68 and 70 patients, respectively, received at least one dose of study drug and were included in the analyses. The frequencies of treatment-related grade 3-5 adverse events up to week 25 were similar in the nivolumab followed by ipilimumab group (34 [50%; 95% CI 37·6-62·4] of 68 patients) and in the ipilimumab followed by nivolumab group (30 [43%; 31·1-55·3] of 70 patients). The most common treatment-related grade 3-4 adverse events during the whole study period were colitis (ten [15%]) in the nivolumab followed by ipilimumab group vs 14 [20%] in the reverse sequence group), increased lipase (ten [15%] vs 12 [17%]), and diarrhoea (eight [12%] vs five [7%]). No treatment-related deaths occurred. The proportion of patients with a response at week 25 was higher with nivolumab followed by ipilimumab than with the reverse sequence (28 [41%; 95% CI 29·4-53·8] vs 14 [20%; 11·4-31·3]). Progression was reported in 26 (38%; 95% CI 26·7-50·8) patients in the nivolumab followed by ipilimumab group and 43 (61%; 49·0-72·8) patients in the reverse sequence group at week 13 and in 26 (38%; 26·7-50·8) and 42 (60%; 47·6-71·5) patients at week 25, respectively. After a median follow-up of 19·8 months (IQR 12·8-25·7), median overall survival was not reached in the nivolumab followed by ipilimumab group (95% CI 23·7-not reached), whereas over a median follow-up of 14·7 months (IQR 5·6-23·9) in the ipilimumab followed by nivolumab group, median overall survival was 16·9 months (95% CI 9·2-26·5; HR 0·48 [95% CI 0·29-0·80]). A higher proportion of patients in the nivolumab followed by ipilimumab group achieved 12-month overall survival than in the ipilimumab followed by nivolumab group (76%; 95% CI 64-85 vs 54%; 42-65).
Interpretation: Nivolumab followed by ipilimumab appears to be a more clinically beneficial option compared with the reverse sequence, albeit with a higher frequency of adverse events.
Funding: Bristol-Myers Squibb.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Sequential immunotherapy regimens-expect the unexpected.Lancet Oncol. 2016 Jul;17(7):854-855. doi: 10.1016/S1470-2045(16)30198-X. Epub 2016 Jun 4. Lancet Oncol. 2016. PMID: 27269742 No abstract available.
References
-
- Wang C, Thudium KB, Han M, et al. In vitro characterization of the anti-PD-1 antibody nivolumab, BMS-936558, and in vivo toxicology in non-human primates. Cancer Immunol Res. 2014;2:846–56. - PubMed
-
- Robert C, Long GV, Brady B, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med. 2015;372:320–30. - PubMed
-
- Weber JS, D'Angelo SP, Minor D, et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2015;16:375–84. - PubMed
-
- Okazaki T, Chikuma S, Iwai Y, Fagarasan S, Honjo T. A rheostat for immune responses: the unique properties of PD-1 and their advantages for clinical application. Nat Immunol. 2013;14:1212–18. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
