

Nivolumab in Patients With Relapsed or Refractory Hematologic Malignancy: Preliminary Results of a Phase Ib Study
- PMID: 27269947
- PMCID: PMC5019749
- DOI: 10.1200/JCO.2015.65.9789
Nivolumab in Patients With Relapsed or Refractory Hematologic Malignancy: Preliminary Results of a Phase Ib Study
Abstract
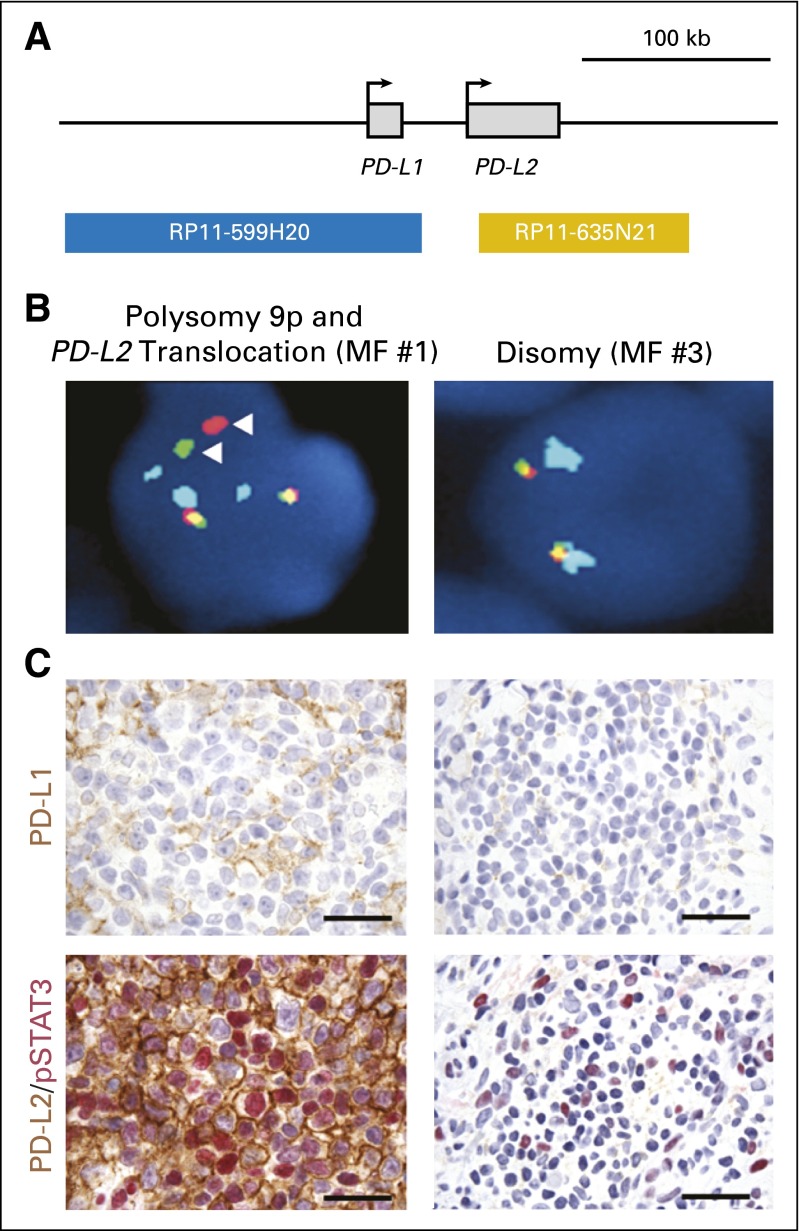
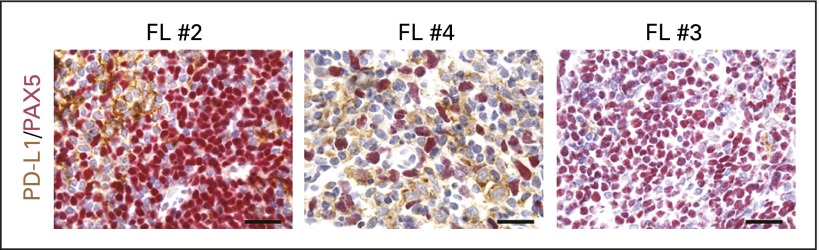
Purpose: Cancer cells can exploit the programmed death-1 (PD-1) immune checkpoint pathway to avoid immune surveillance by modulating T-lymphocyte activity. In part, this may occur through overexpression of PD-1 and PD-1 pathway ligands (PD-L1 and PD-L2) in the tumor microenvironment. PD-1 blockade has produced significant antitumor activity in solid tumors, and similar evidence has emerged in hematologic malignancies.
Methods: In this phase I, open-label, dose-escalation, cohort-expansion study, patients with relapsed or refractory B-cell lymphoma, T-cell lymphoma, and multiple myeloma received the anti-PD-1 monoclonal antibody nivolumab at doses of 1 or 3 mg/kg every 2 weeks. This study aimed to evaluate the safety and efficacy of nivolumab and to assess PD-L1/PD-L2 locus integrity and protein expression.
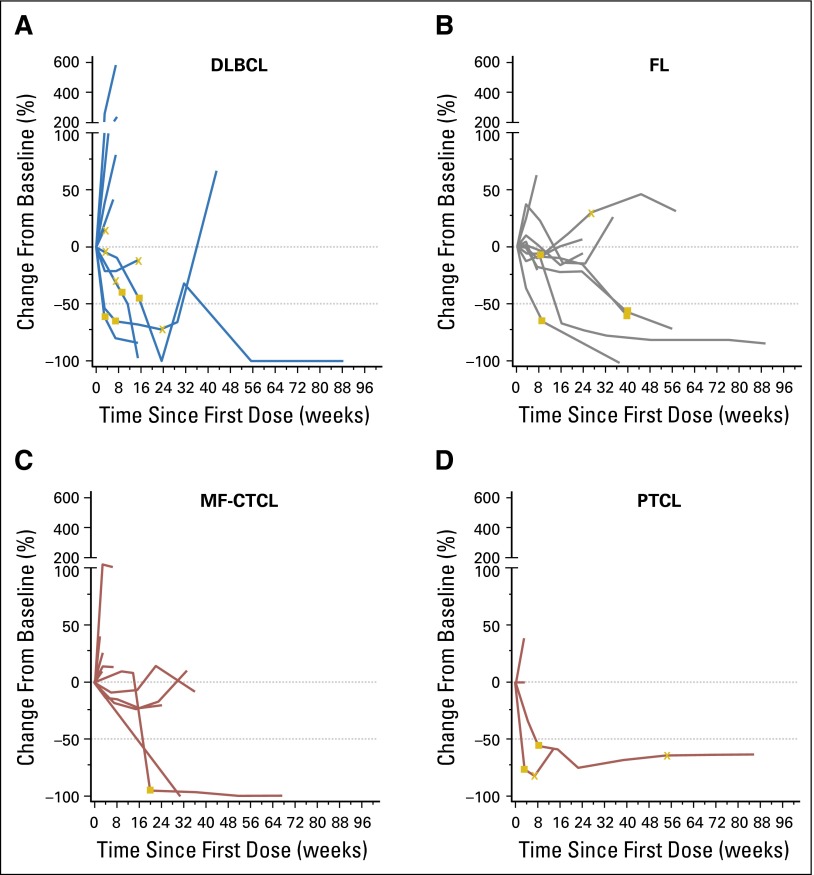
Results: Eighty-one patients were treated (follicular lymphoma, n = 10; diffuse large B-cell lymphoma, n = 11; other B-cell lymphomas, n = 10; mycosis fungoides, n = 13; peripheral T-cell lymphoma, n = 5; other T-cell lymphomas, n = 5; multiple myeloma, n = 27). Patients had received a median of three (range, one to 12) prior systemic treatments. Drug-related adverse events occurred in 51 (63%) patients, and most were grade 1 or 2. Objective response rates were 40%, 36%, 15%, and 40% among patients with follicular lymphoma, diffuse large B-cell lymphoma, mycosis fungoides, and peripheral T-cell lymphoma, respectively. Median time of follow-up observation was 66.6 weeks (range, 1.6 to 132.0+ weeks). Durations of response in individual patients ranged from 6.0 to 81.6+ weeks.
Conclusion: Nivolumab was well tolerated and exhibited antitumor activity in extensively pretreated patients with relapsed or refractory B- and T-cell lymphomas. Additional studies of nivolumab in these diseases are ongoing.
Trial registration: ClinicalTrials.gov NCT01592370.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article.
Figures
References
-
- Andorsky DJ, Yamada RE, Said J, et al. Programmed death ligand 1 is expressed by non-Hodgkin lymphomas and inhibits the activity of tumor-associated T cells. Clin Cancer Res. 2011;17:4232–4244. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
