

Age- and Tumor Subtype-Specific Breast Cancer Risk Estimates for CHEK2*1100delC Carriers
- PMID: 27269948
- PMCID: PMC5019754
- DOI: 10.1200/JCO.2016.66.5844
Age- and Tumor Subtype-Specific Breast Cancer Risk Estimates for CHEK2*1100delC Carriers
Abstract
Purpose: CHEK2*1100delC is a well-established breast cancer risk variant that is most prevalent in European populations; however, there are limited data on risk of breast cancer by age and tumor subtype, which limits its usefulness in breast cancer risk prediction. We aimed to generate tumor subtype- and age-specific risk estimates by using data from the Breast Cancer Association Consortium, including 44,777 patients with breast cancer and 42,997 controls from 33 studies genotyped for CHEK2*1100delC.
Patients and methods: CHEK2*1100delC genotyping was mostly done by a custom Taqman assay. Breast cancer odds ratios (ORs) for CHEK2*1100delC carriers versus noncarriers were estimated by using logistic regression and adjusted for study (categorical) and age. Main analyses included patients with invasive breast cancer from population- and hospital-based studies.
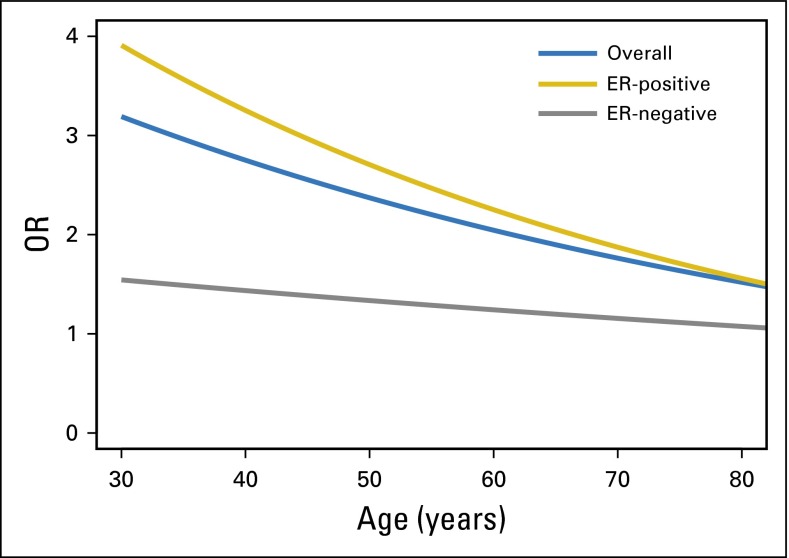
Results: Proportions of heterozygous CHEK2*1100delC carriers in controls, in patients with breast cancer from population- and hospital-based studies, and in patients with breast cancer from familial- and clinical genetics center-based studies were 0.5%, 1.3%, and 3.0%, respectively. The estimated OR for invasive breast cancer was 2.26 (95%CI, 1.90 to 2.69; P = 2.3 × 10(-20)). The OR was higher for estrogen receptor (ER)-positive disease (2.55 [95%CI, 2.10 to 3.10; P = 4.9 × 10(-21)]) than it was for ER-negative disease (1.32 [95%CI, 0.93 to 1.88; P = .12]; P interaction = 9.9 × 10(-4)). The OR significantly declined with attained age for breast cancer overall (P = .001) and for ER-positive tumors (P = .001). Estimated cumulative risks for development of ER-positive and ER-negative tumors by age 80 in CHEK2*1100delC carriers were 20% and 3%, respectively, compared with 9% and 2%, respectively, in the general population of the United Kingdom.
Conclusion: These CHEK2*1100delC breast cancer risk estimates provide a basis for incorporating CHEK2*1100delC into breast cancer risk prediction models and into guidelines for intensified screening and follow-up.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article.
Figures





References
Publication types
MeSH terms
Substances
Grants and funding
- MC_PC_14105/MRC_/Medical Research Council/United Kingdom
- R01 CA176785/CA/NCI NIH HHS/United States
- UM1 CA164920/CA/NCI NIH HHS/United States
- 11174/CRUK_/Cancer Research UK/United Kingdom
- 16565/CRUK_/Cancer Research UK/United Kingdom
- R01 CA058860/CA/NCI NIH HHS/United States
- 20861/CRUK_/Cancer Research UK/United Kingdom
- K07 CA092044/CA/NCI NIH HHS/United States
- U01 CA116167/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- P50 CA116201/CA/NCI NIH HHS/United States
- C1287/A12014/CRUK_/Cancer Research UK/United Kingdom
- U01 CA058860/CA/NCI NIH HHS/United States
- 090532/Z/09/Z/WT_/Wellcome Trust/United Kingdom
- C1287/A10118/CRUK_/Cancer Research UK/United Kingdom
- R01 CA047305/CA/NCI NIH HHS/United States
- R01 CA047147/CA/NCI NIH HHS/United States
- R01 CA116167/CA/NCI NIH HHS/United States
- 10119/CRUK_/Cancer Research UK/United Kingdom
- R01 CA069664/CA/NCI NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- 10118/CRUK_/Cancer Research UK/United Kingdom
- R01 CA192393/CA/NCI NIH HHS/United States
- 16561/CRUK_/Cancer Research UK/United Kingdom
- 10124/CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
