

Ameloblastoma: 25 Year Experience at a Single Institution
- PMID: 27272180
- PMCID: PMC5082058
- DOI: 10.1007/s12105-016-0734-5
Ameloblastoma: 25 Year Experience at a Single Institution
Abstract
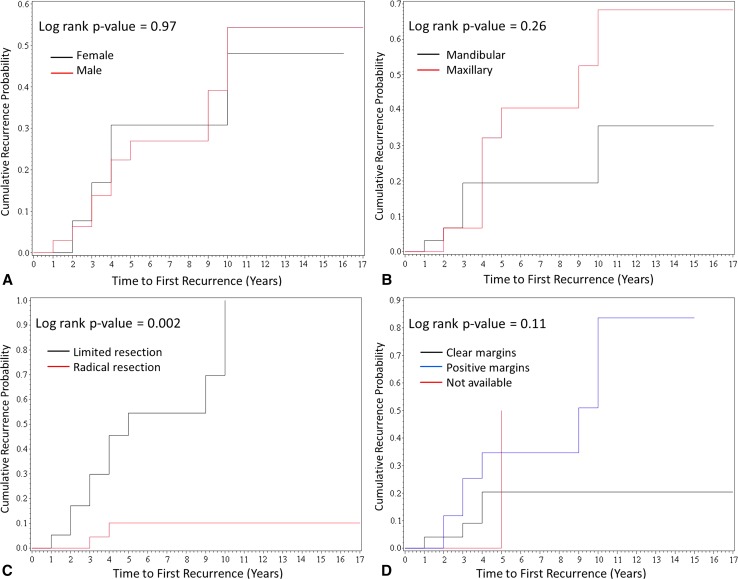
Ameloblastoma is a rare, locally aggressive odontogenic neoplasm, accounting for fewer than 1 % of head and neck tumors. Recent literature suggests that the initial surgical approach and histologic growth patterns are the most important prognostic determinants in ameloblastoma. The aim of this study was to compare the clinical presentation, management, and outcomes of patients with ameloblastoma with data reported in the literature; the study spanned 2 decades at a single institution. The institution's database was searched for all patients with pathologically confirmed ameloblastoma, diagnosed between 1990 and 2015. The data collected included sex, age, clinical and imaging findings, management, histologic pattern, clearance of surgical margins, length of follow-up, time to recurrence, and disease-related mortality. The potential risk factors of recurrence were evaluated using log-rank test, proportional hazard model, and Fisher exact test. Review of the database yielded 54 patients with pathologically confirmed ameloblastoma and follow-up. Recurrence was noted in 13 (24 %) patients. Surgical approach was associated with the risk of recurrence (6.1 % following radical resection vs. 52 % following limited surgery, p = 0.002). There were trends toward higher recurrence rate in the group with pathologically documented positive margins (p = 0.054) and in follicular ameloblastoma (p = 0.35). Transformation into ameloblastic carcinoma was identified in two patients. There was no disease-related mortality. Our study confirms the recent data regarding the importance of radical surgical resection in management of ameloblastoma. Surgical approach appears to be the strongest predictor of tumor clearance.
Keywords: Ameloblastoma; Ameloblastoma histologic pattern; Ameloblastoma management; Ameloblastoma pathology; Ameloblastoma prognosis; Ameloblastoma recurrence.
Conflict of interest statement
The authors declare that they have no conflict of interest. Ethical Approval This study was approved by the Hospital of University of Pennsylvania Ethics Committee (IRB). For this type of study formal consent was not required.
Figures
References
-
- Barnes L, Eveson JW, Reichart P, Sidransky D. World Health Organization classification of tumors. Pathology and genetics of head and neck tumours. Lyon: IARC Press; 2005.
-
- McClary AC, West RB, McClary AC, Pollack JR, Fischbein NJ, Holsinger CF, Sunwoo J, Colevas AD, Sirjani D. Ameloblastoma: a clinical review and trends in management. Eur Arch Otorhinolaryngol. 2015 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
