

Study of the Atopic March: Development of Atopic Comorbidities
- PMID: 27273433
- PMCID: PMC5649252
- DOI: 10.1111/pde.12867
Study of the Atopic March: Development of Atopic Comorbidities
Abstract
Background: Atopic dermatitis (AD) is often the first step in the atopic march leading to the development of asthma or allergic rhinitis. The goal of this study was to determine whether early intervention with pimecrolimus limits the atopic march in infants with AD and to evaluate its efficacy and safety.
Methods: This was a 3-year double-blind study in which patients were randomized to pimecrolimus or vehicle and then open-label pimecrolimus for a planned further 3 years. Rescue topical corticosteroid was permitted if 3 days of study medication led to no improvement; investigators made decisions on rescue medication until week 14 and caregivers thereafter. Efficacy assessments included disease-free days, Eczema Area and Severity Index, and body surface area affected.
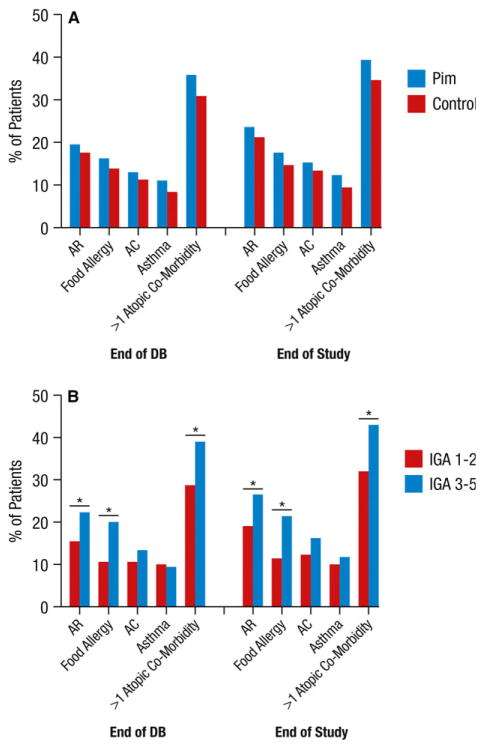
Results: Infants ages 3 to 18 months with recent-onset AD (≤3 months) were observed for a mean of 2.8 years (N = 1,091). No significant differences between pimecrolimus- and placebo-treated groups were found in the percentage of patients with AD who developed asthma (10.7%) or other allergic conditions (allergic rhinitis, 22.4%; food allergy, 15.9%; allergic conjunctivitis, 14.1%; one or more atopic comorbidities, 37.0%) by study end. Allergic rhinitis, food allergy, and having one or more atopic comorbidities (but not asthma or allergic conjunctivitis alone) developed significantly more often in infants with greater AD severity at baseline. Pimecrolimus was significantly more effective than vehicle for AD treatment at week 14. Adverse event incidences were similar.
Conclusions: This longitudinal observation of infants with AD provides evidence of the atopic march. Pimecrolimus was safe and effective in infants with mild to moderate AD.
© 2016 Wiley Periodicals, Inc.
Conflict of interest statement
All authors except Rada Dakovic were past investigators for Novartis. Lynda Schneider is an investigator for Astellas. Jon Hanifin is a consultant with honorarium for Novartis and an investigator for Astellas. Lawrence F. Eichenfield is an investigator for Astellas, a consultant with honorarium for Valeant, and a past consultant with honorarium for Novartis. Jonathan M. Spergel is a consultant with honorarium for Novartis, Dannone, and DBV Technologies. Rada Dakovic is a Meda Pharma employee. Amy S. Paller is a consultant with honorarium for Novartis and an investigator for Astellas.
Figures


References
-
- Spergel JM. From atopic dermatitis to asthma: the atopic march. Ann Allergy Asthma Immunol. 2010;105:99–106. - PubMed
-
- Galli E, Gianni S, Auricchio G, et al. Atopic dermatitis and asthma. Allergy Asthma Proc. 2007;28:540–543. - PubMed
-
- Paul C, Cork M, Rossi AB, et al. Safety and tolerability of 1% pimecrolimus cream among infants: experience with 1133 patients treated for up to 2 years. Pediatrics. 2006;117:e118–e128. - PubMed
-
- Sigurgeirsson B, Boznanski A, Todd G, et al. Safety and efficacy of pimecrolimus in atopic dermatitis: a 5-year randomized trial. Pediatrics. 2015;135:597–606. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
