

Intensive Treatment and Severe Hypoglycemia Among Adults With Type 2 Diabetes
- PMID: 27273792
- PMCID: PMC5380118
- DOI: 10.1001/jamainternmed.2016.2275
Intensive Treatment and Severe Hypoglycemia Among Adults With Type 2 Diabetes
Abstract
Importance: Intensive glucose-lowering treatment among patients with non-insulin-requiring type 2 diabetes may increase the risk of hypoglycemia.
Objectives: To estimate the prevalence of intensive treatment and the association between intensive treatment, clinical complexity, and incidence of severe hypoglycemia among adults with type 2 diabetes who are not using insulin.
Design, setting, and participants: Retrospective analysis of administrative, pharmacy, and laboratory data from the OptumLabs Data Warehouse from January 1, 2001, through December 31, 2013. The study included nonpregnant adults 18 years or older with type 2 diabetes who achieved and maintained a hemoglobin A1c (HbA1c) level less than 7.0% without use of insulin and had no episodes of severe hypoglycemia or hyperglycemia in the prior 12 months.
Main outcomes and measures: Risk-adjusted probability of intensive treatment and incident severe hypoglycemia, stratified by patient clinical complexity. Intensive treatment was defined as use of more glucose-lowering medications than recommended by practice guidelines at specific index HbA1c levels. Severe hypoglycemia was ascertained by ambulatory, emergency department, and hospital claims for hypoglycemia during the 2 years after the index HbA1c test. Patients were categorized as having high vs low clinical complexity if they were 75 years or older, had dementia or end-stage renal disease, or had 3 or more serious chronic conditions.
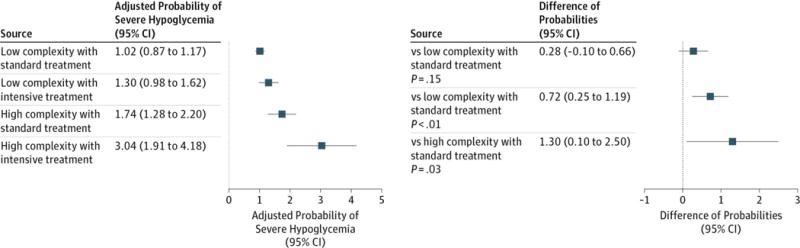
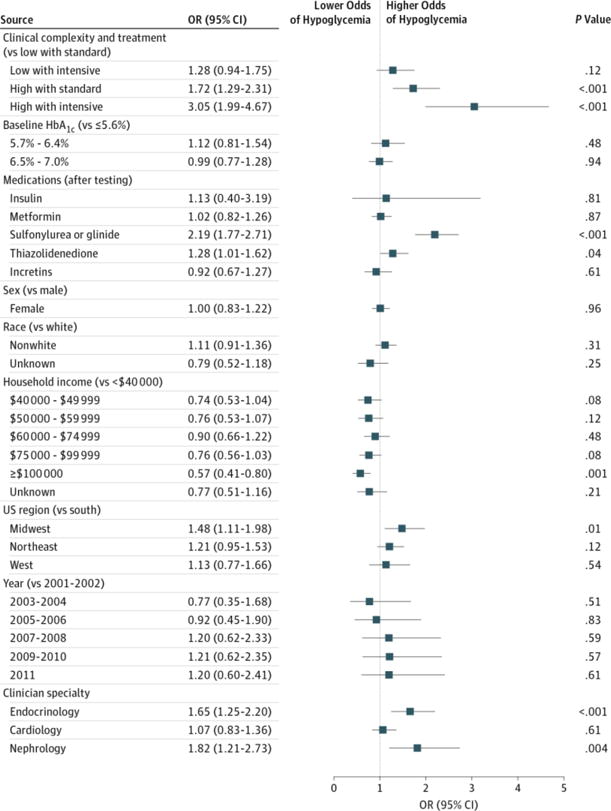
Results: Of 31 542 eligible patients (median age, 58 years; interquartile range, 51-65 years; 15 483 women [49.1%]; 18 188 white [57.7%]), 3910 (12.4%) had clinical complexity. The risk-adjusted probability of intensive treatment was 25.7% (95% CI, 25.1%-26.2%) in patients with low clinical complexity and 20.8% (95% CI, 19.4%-22.2%) in patients with high clinical complexity. In patients with low clinical complexity, the risk-adjusted probability of severe hypoglycemia during the subsequent 2 years was 1.02% (95% CI, 0.87%-1.17%) with standard treatment and 1.30% (95% CI, 0.98%-1.62%) with intensive treatment (absolute difference, 0.28%; 95% CI, -0.10% to 0.66%). In patients with high clinical complexity, intensive treatment significantly increased the risk-adjusted probability of severe hypoglycemia from 1.74% (95% CI, 1.28%-2.20%) with standard treatment to 3.04% (95% CI, 1.91%-4.18%) with intensive treatment (absolute difference, 1.30%; 95% CI, 0.10%-2.50%).
Conclusions and relevance: More than 20% of patients with type 2 diabetes received intensive treatment that may be unnecessary. Among patients with high clinical complexity, intensive treatment nearly doubles the risk of severe hypoglycemia.
Conflict of interest statement
Figures

Comment in
-
Deintensification of Routine Medical Services: The Next Frontier for Improving Care Quality.JAMA Intern Med. 2016 Jul 1;176(7):978-80. doi: 10.1001/jamainternmed.2016.2292. JAMA Intern Med. 2016. PMID: 27272959 No abstract available.
References
-
- Turnbull FM, Abraira C, Anderson RJ, et al. Control Group Intensive glucose control and macrovascular outcomes in type 2 diabetes [published correction appears in Diabetologia. 2009;52(1):2470] Diabetologia. 2009;52(11):2288–2298. - PubMed
-
- Zoungas S, Patel A, Chalmers J, et al. ADVANCE Collaborative Group Severe hypoglycemia and risks of vascular events and death. N Engl J Med. 2010;363(15):1410–1418. - PubMed
-
- Duckworth W, Abraira C, Moritz T, et al. VADT Investigators Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. 2009;360(2):129–139. - PubMed
-
- Duckworth WC, Abraira C, Moritz TE, et al. Investigators of the VADT The duration of diabetes affects the response to intensive glucose control in type 2 subjects: the VA Diabetes Trial. J Diabetes Complications. 2011;25(6):355–361. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
