

Prolonged length of stay associated with air leak following pulmonary resection has a negative impact on hospital margin
- PMID: 27274293
- PMCID: PMC4876678
- DOI: 10.2147/CEOR.S95603
Prolonged length of stay associated with air leak following pulmonary resection has a negative impact on hospital margin
Erratum in
-
Erratum: Prolonged length of stay associated with air leak following pulmonary resection has a negative impact on hospital margin [Erratum].Clinicoecon Outcomes Res. 2016 Jul 15;8:351. doi: 10.2147/CEOR.S113233. eCollection 2016. Clinicoecon Outcomes Res. 2016. PMID: 27471401 Free PMC article.
Abstract
Background: Protracted hospitalizations due to air leaks following lung resections are a significant source of morbidity and prolonged hospital length of stay (LOS), with potentially significant impact on hospital margins. This study aimed to evaluate the relationship between air leaks, LOS, and financial outcomes among discharges following lung resections.
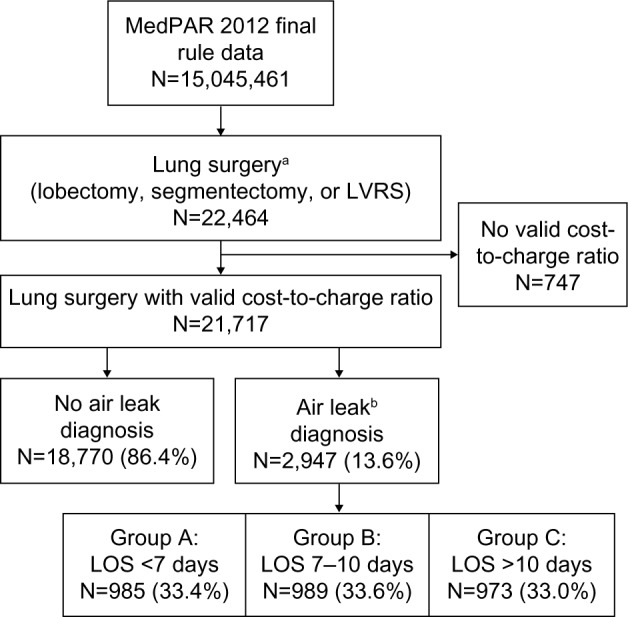
Materials and methods: The Medicare Provider Analysis and Review file for fiscal year 2012 was utilized to identify inpatient hospital discharges that recorded International Classification of Diseases (ICD-9) procedure codes for lobectomy, segmentectomy, and lung volume reduction surgery (n=21,717). Discharges coded with postoperative air leaks (ICD-9-CM codes 512.2 and 512.84) were defined as the air leak diagnosis group (n=2,947), then subcategorized by LOS: 1) <7 days; 2) 7-10 days; and 3) ≥11 days. Median hospital charges, costs, payments, and payment-to-cost ratios were compared between non-air leak and air leak groups, and across LOS subcategories.
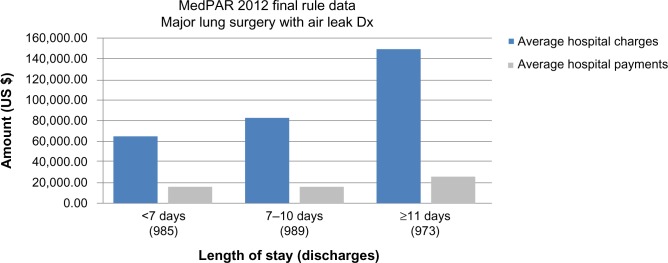
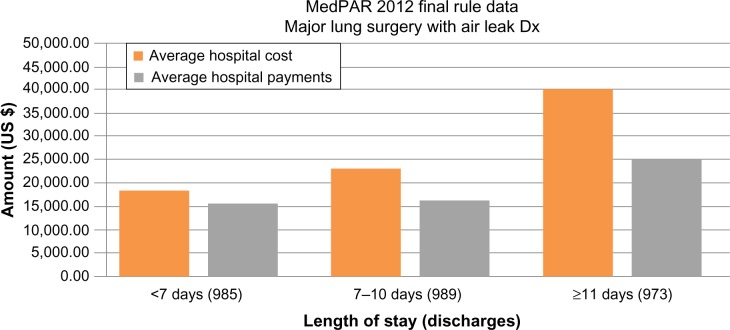
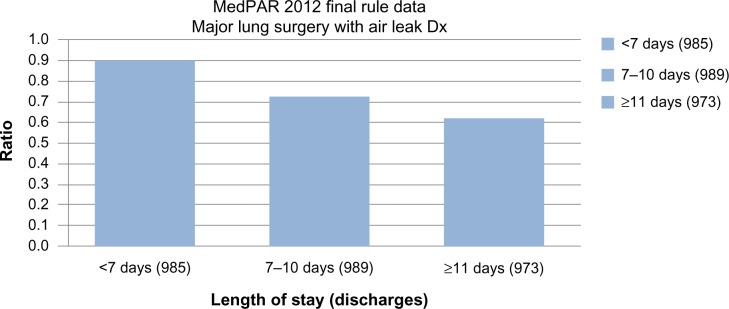
Results: For identified patients, hospital charges, costs, and payments were significantly greater among patients with air leak diagnoses compared to patients without (P<0.001). Hospital charges and costs increased substantially with prolonged LOS, but were not matched by a proportionate increase in hospital payments. Patients with LOS <7, 7-10, and ≥11 days had median hospital charges of US $57,129, $73,572, and $115,623, and costs of $17,594, $21,711, and $33,786, respectively. Hospital payment increases were substantially lower at $16,494, $16,307, and $19,337, respectively. The payment-to-cost ratio significantly lowered with each LOS increase (P<0.001). Higher inpatient hospital mortality was observed among the LOS ≥11 days subgroup compared with the LOS <11 days subgroup (P<0.001).
Conclusion: Patients who develop prolonged air leaks after lobectomy, segmentectomy, or lung volume reduction surgery have the best clinical and financial outcomes. Hospitals experience markedly lower payment-to-cost ratios as LOS increases. Interventions minimizing air leak or allowing outpatient management will improve financial performance and hospital margins for lung surgery.
Keywords: air leaks; hospital financials; length of stay.
Figures
References
-
- Bille A, Borasio P, Gisabella M, et al. Air leaks following pulmonary resection for malignancy: risk factors, qualitative and quantitative analysis. Interact Cardiovasc Thorac Surg. 2011;13(1):11–15. - PubMed
-
- Brunelli A, Xiume F, Al Refai M, Salati M, Marasco R, Sabbatini A. Air leaks after lobectomy increase the risk of empyema but not of cardiopulmonary complications: a case-matched analysis. Chest. 2006;130(4):1150–1156. - PubMed
-
- DeCamp MM, Blackstone EH, Naunheim KS, et al. Patient and surgical factors influencing air leak after lung volume reduction surgery: lessons learned from the National Emphysema Treatment Trial. Ann Thorac Surg. 2006;82(1):197–206. discussion 206–207. - PubMed
-
- Bardell T, Petsikas D. What keeps postpulmonary resection patients in hospital? Can Respir J. 2003;10(2):86–89. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
