

Suppository naproxen reduces incidence and severity of post-endoscopic retrograde cholangiopancreatography pancreatitis: Randomized controlled trial
- PMID: 27275104
- PMCID: PMC4886387
- DOI: 10.3748/wjg.v22.i21.5114
Suppository naproxen reduces incidence and severity of post-endoscopic retrograde cholangiopancreatography pancreatitis: Randomized controlled trial
Abstract
Aim: To determine the efficacy of rectally administered naproxen for the prevention of post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis (PEP).
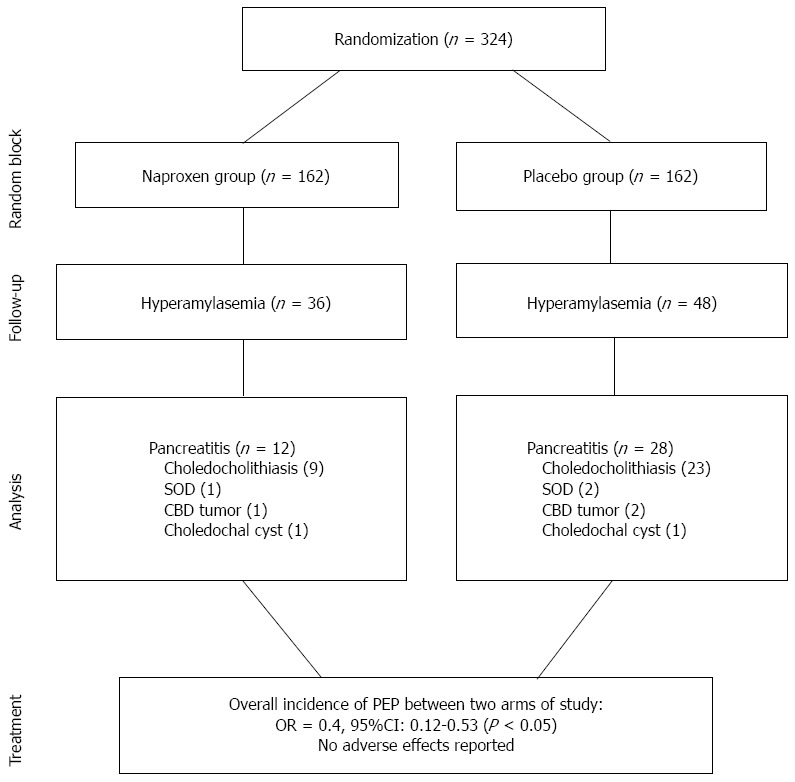
Methods: This double-blind randomized control trial conducted from January 2013 to April 2014 at the Gastrointestinal and Liver Diseases Research Center in Rasht, Iran. A total of 324 patients were selected from candidates for diagnostic or therapeutic ERCP by using the simple sampling method. Patients received a single dose of Naproxen (500 mg; n = 162) or a placebo (n = 162) per rectum immediately before ERCP. The overall incidence of PEP, incidence of mild to severe PEP, serum amylase levels and adverse effects were measured. The primary outcome measure was the development of pancreatitis onset of pain in the upper abdomen and elevation of the serum amylase level to > 3 × the upper normal limit (60-100 IU/L) within 24 h after ERCP. The severity of PEP was classified according to the duration of therapeutic intervention for PEP: mild, 2-3 d; moderate 4-10 d; and severe, > 10 d and/or necessitated surgical or intensive treatment, or contributed to death.
Results: PEP occurred in 12% (40/324) of participants, and was significantly more frequent in the placebo group compared to the naproxen group (P < 0.01). Of the participants, 25.9% (84/324) developed hyperamylasemia within 2 h of procedure completion, among whom only 35 cases belonged to the naproxen group (P < 0.01). The incidence of PEP was significantly higher in female sex, in patients receiving pancreatic duct injection, more than 3 times pancreatic duct cannulations, and ERCP duration more than 40 min (Ps < 0.01). There were no statistically significant differences between the groups regarding the procedures or factors that might increase the risk of PEP, sphincterotomy, precut requirement, biliary duct injection and number of pancreatic duct cannulations. In the subgroup of patients with pancreatic duct injection, the rate of pancreatitis in the naproxen group was significantly lower than that in the placebo (6 patients vs 23 patients, P < 0.01, RRR = 12%, AR = 0.3, 95%CI: 0.2-0.6). Naproxen reduced the PEP in patients with ≥ 3 pancreatic cannulations (P < 0.01, RRR = 25%, AR = 0.1, 95%CI: 0.1-0.4) and an ERCP duration > 40 min (P < 0.01, RRR = 20%, AR = 0.9, 95%CI: 0.4-1.2).
Conclusion: Single dose of suppository naproxen administered immediately before ERCP reduces the incidence of PEP.
Keywords: Naproxen; Nonsteroidal anti-inflammatory drugs; Pancreatic duct injection; Pancreatitis; Post-endoscopic retrograde cholangiopancreatography; Serum amylase.
Figures
References
-
- Rabenstein T, Hahn EG. Post-ERCP pancreatitis: new momentum. Endoscopy. 2002;34:325–329. - PubMed
-
- Freeman ML, Guda NM. Prevention of post-ERCP pancreatitis: a comprehensive review. Gastrointest Endosc. 2004;59:845–864. - PubMed
-
- Shi N, Deng L, Altaf K, Huang W, Xue P, Xia Q. Rectal indomethacin for the prevention of post-ERCP pancreatitis: A meta-analysis of randomized controlled trials. Turk J Gastroenterol. 2015;26:236–240. - PubMed
-
- Kochar B, Akshintala VS, Afghani E, Elmunzer BJ, Kim KJ, Lennon AM, Khashab MA, Kalloo AN, Singh VK. Incidence, severity, and mortality of post-ERCP pancreatitis: a systematic review by using randomized, controlled trials. Gastrointest Endosc. 2015;81:143–149.e9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
