

Endovascular Treatment of Multilevel Chronic Total Occlusion Using a Stent Puncture Technique in Buerger's Disease
- PMID: 27275180
- PMCID: PMC4891608
- DOI: 10.4070/kcj.2016.46.3.417
Endovascular Treatment of Multilevel Chronic Total Occlusion Using a Stent Puncture Technique in Buerger's Disease
Abstract
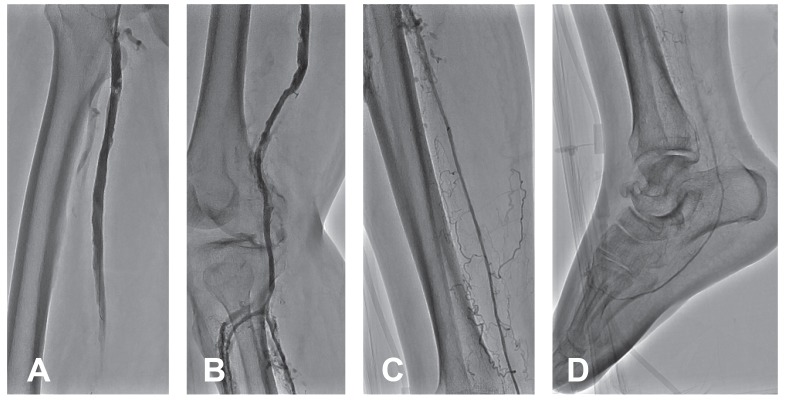
We reported a patient with Buerger's disease who presented with critical limb ischemiawith prior recurrent occlusions after multiple surgical and endovascular treatments. Total occlusion of the whole native femoropopliteal and infrapopliteal arteries was observed. The femoropopliteal bypass graft, as well as a stent that was implanted in the mid-popliteal artery, were also occluded. Because of the lack of distal targets for bypass, surgical revascularization was not feasible; therefore, we decided to perform endovascular treatment. To overcome the limitation of vascular access, the previously implanted popliteal stent was directly punctured, and a guide wire was passed through the bypass graft. After the organized thrombus in the bypass graft was aspirated, further recanalization below the popliteal stent down to the plantar arteries was performed successfully. In conclusion, the stent puncture technique is a feasible and safe option for overcoming the limitations of vascular access in patients with multilevel occlusions.
Keywords: Endovascular procedures; Peripheral artery disease; Punctures; Stents; Thromboangiitis obliterans.
Figures




References
-
- Olin JW. Thromboangiitis obliterans (Buerger's disease) N Engl J Med. 2000;343:864–869. - PubMed
-
- Sasaki S, Sakuma M, Kunihara T, Yasuda K. Distribution of arterial involvement in thromboangiitis obliterans (Buerger's disease): results of a study conducted by the Intractable Vasculitis Syndromes Research Group in Japan. Surg Today. 2000;30:600–605. - PubMed
-
- Graziani L, Morelli L, Parini F, et al. Clinical outcome after extended endovascular recanalization in Buerger's disease in 20 consecutive cases. Ann Vasc Surg. 2012;26:387–395. - PubMed
-
- Laird JR, Katzen BT, Scheinert D, et al. Nitinol stent implantation versus balloon angioplasty for lesions in the superficial femoral artery and proximal popliteal artery: twelve-month results from the RESILIENT randomized trial. Circ Cardiovasc Interv. 2010;3:267–276. - PubMed
-
- Schlager O, Dick P, Sabeti S, et al. Long-segment SFA stenting--the dark sides: in-stent restenosis, clinical deterioration, and stent fractures. J Endovasc Ther. 2005;12:676–684. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
