Achieving Higher Diagnostic Results in Stereotactic Brain Biopsy by Simple and Novel Technique
- PMID: 27275204
- PMCID: PMC4877797
- DOI: 10.3889/oamjms.2015.016
Achieving Higher Diagnostic Results in Stereotactic Brain Biopsy by Simple and Novel Technique
Abstract
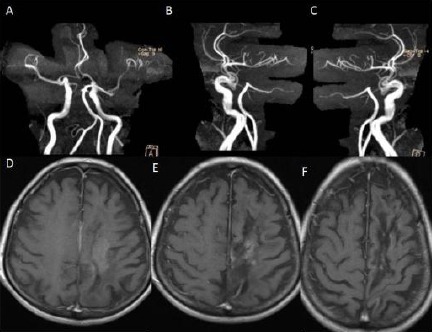
Background: Neurosurgeons have preferred to perform the stereotactic biopsy for pathologic diagnosis when the intracranial pathology located eloquent areas and deep sites of the brain.
Aim: To get a higher ratio of definite pathologic diagnosis during stereotactic biopsy and develop practical method.
Material and methods: We determined at least two different target points and two different trajectories to take brain biopsy during stereotactic biopsy. It is a different way from the conventional stereotactic biopsy method in which one point has been selected to take a biopsy. We separated our patients into two groups, group 1 (N=10), and group 2 (N= 19). We chose one target to take a biopsy in group 1, and two different targets and two different trajectories in group 2. In group 2, one patient underwent craniotomy due to hemorrhage at the site of the biopsy during tissue biting. However, none of the patients in both groups suffered any neurological complication related biopsy procedure.
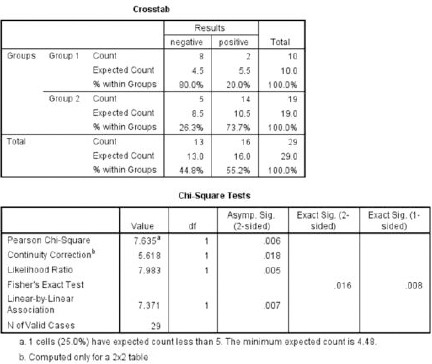
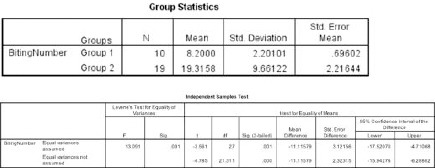
Results: In group 1, two of 10 cases, and, in group 2, fourteen of 19 cases had positive biopsy harvesting. These results showed statistically significant difference between group 1 and group 2 (P<0.05).
Conclusions: Regarding these results, choosing more than one trajectories and taking at least six specimens from each target provides higher diagnostic rate in stereotaxic biopsy taking method.
Keywords: Brain Tumour; Diagnostic rate; Diffuse infilitrative; Eloquent Areas; Stereotactic Biopsy.
Figures
References
-
- Apuzzo ML, Sabshin JK. Computed tomographic guidance stereotaxis in the management of intracranial mass lesions. Neurosurgery. 1983;12:277–85. - PubMed
-
- Ostertag CB, Mennel HD, Kiessling M. Stereotactic biopsy of brain tumors. Surg Neurol. 1980;14:275–83. - PubMed
-
- Edner G. Stereotactic biopsy of intracranial space occupying lesions. Acta Neurochir (Wien) 1981;57:213–34. - PubMed
-
- Grunert P, Ungersbock K, Bohl J, Kitz K, Hopf N. Results of 200 intracranial stereotactic biopsies. Neurosurgery. 1994;17:59–66. - PubMed
-
- Hall WA. The safety and efficacy of stereotactic biopsy for intracranial lesions. Cancer. 1998;82:1749–55. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources