

Intensive Blood-Pressure Lowering in Patients with Acute Cerebral Hemorrhage
- PMID: 27276234
- PMCID: PMC5345109
- DOI: 10.1056/NEJMoa1603460
Intensive Blood-Pressure Lowering in Patients with Acute Cerebral Hemorrhage
Abstract
Background: Limited data are available to guide the choice of a target for the systolic blood-pressure level when treating acute hypertensive response in patients with intracerebral hemorrhage.
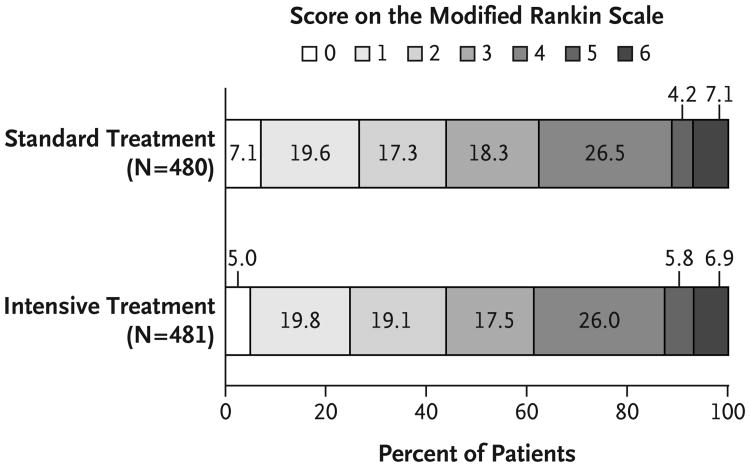
Methods: We randomly assigned eligible participants with intracerebral hemorrhage (volume, <60 cm(3)) and a Glasgow Coma Scale (GCS) score of 5 or more (on a scale from 3 to 15, with lower scores indicating worse condition) to a systolic blood-pressure target of 110 to 139 mm Hg (intensive treatment) or a target of 140 to 179 mm Hg (standard treatment) in order to test the superiority of intensive reduction of systolic blood pressure to standard reduction; intravenous nicardipine to lower blood pressure was administered within 4.5 hours after symptom onset. The primary outcome was death or disability (modified Rankin scale score of 4 to 6, on a scale ranging from 0 [no symptoms] to 6 [death]) at 3 months after randomization, as ascertained by an investigator who was unaware of the treatment assignments.
Results: Among 1000 participants with a mean (±SD) systolic blood pressure of 200.6±27.0 mm Hg at baseline, 500 were assigned to intensive treatment and 500 to standard treatment. The mean age of the patients was 61.9 years, and 56.2% were Asian. Enrollment was stopped because of futility after a prespecified interim analysis. The primary outcome of death or disability was observed in 38.7% of the participants (186 of 481) in the intensive-treatment group and in 37.7% (181 of 480) in the standard-treatment group (relative risk, 1.04; 95% confidence interval, 0.85 to 1.27; analysis was adjusted for age, initial GCS score, and presence or absence of intraventricular hemorrhage). Serious adverse events occurring within 72 hours after randomization that were considered by the site investigator to be related to treatment were reported in 1.6% of the patients in the intensive-treatment group and in 1.2% of those in the standard-treatment group. The rate of renal adverse events within 7 days after randomization was significantly higher in the intensive-treatment group than in the standard-treatment group (9.0% vs. 4.0%, P=0.002).
Conclusions: The treatment of participants with intracerebral hemorrhage to achieve a target systolic blood pressure of 110 to 139 mm Hg did not result in a lower rate of death or disability than standard reduction to a target of 140 to 179 mm Hg. (Funded by the National Institute of Neurological Disorders and Stroke and the National Cerebral and Cardiovascular Center; ATACH-2 ClinicalTrials.gov number, NCT01176565 .).
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures


Comment in
-
Blood pressure in acute intra-cerebral hemorrhage.Ann Transl Med. 2016 Aug;4(16):320. doi: 10.21037/atm.2016.08.04. Ann Transl Med. 2016. PMID: 27668240 Free PMC article. No abstract available.
-
Intensive lowering of blood pressure in acute intracerebral haemorrhage: Where do we stand today?Natl Med J India. 2016 May-Jun;29(3):153-154. Natl Med J India. 2016. PMID: 27808065 No abstract available.
-
A Randomized Clinical Trial of Aggressive Blood Pressure Control in Patients With Acute Cerebral Hemorrhage.Neurosurgery. 2016 Dec;79(6):N17-N18. doi: 10.1227/01.neu.0000508604.61565.ba. Neurosurgery. 2016. PMID: 27861410 No abstract available.
-
Intensive Blood-Pressure Lowering in Cerebral Hemorrhage.N Engl J Med. 2016 Dec 8;375(23):e48. doi: 10.1056/NEJMc1613117. N Engl J Med. 2016. PMID: 27959682 No abstract available.
-
Intensive Blood-Pressure Lowering in Cerebral Hemorrhage.N Engl J Med. 2016 Dec 8;375(23):e48. doi: 10.1056/NEJMc1613117. N Engl J Med. 2016. PMID: 27959683 No abstract available.
-
Intensive Blood-Pressure Lowering in Cerebral Hemorrhage.N Engl J Med. 2016 Dec 8;375(23):e48. doi: 10.1056/NEJMc1613117. N Engl J Med. 2016. PMID: 28112901 No abstract available.
-
Intensive Blood-Pressure Lowering in Cerebral Hemorrhage.N Engl J Med. 2016 Dec 8;375(23):e48. doi: 10.1056/NEJMc1613117. N Engl J Med. 2016. PMID: 28112902 No abstract available.
-
Intensive blood pressure lowering provides no additional benefits and results in more adverse events.Evid Based Med. 2017 Jun;22(3):102. doi: 10.1136/ebmed-2016-110594. Epub 2017 May 25. Evid Based Med. 2017. PMID: 28546145 No abstract available.
-
Intensive blood-pressure lowering in patients with acute cerebral hemorrhage.CJEM. 2018 Mar;20(2):256-259. doi: 10.1017/cem.2017.35. Epub 2017 Jun 9. CJEM. 2018. PMID: 28595677
-
Updates in Stroke Care.Am J Respir Crit Care Med. 2018 May 15;197(10):1340-1343. doi: 10.1164/rccm.201702-0413RR. Am J Respir Crit Care Med. 2018. PMID: 29566534 No abstract available.
References
-
- Qureshi AI. The importance of acute hypertensive response in ICH. Stroke. 2013;44(1):S67–9. - PubMed
-
- Dandapani BK, Suzuki S, Kelley RE, Reyes-Iglesias Y, Duncan RC. Relation between blood pressure and outcome in intracerebral hemorrhage. Stroke. 1995;26:21–4. - PubMed
-
- Anderson CS, Huang Y, Arima H, et al. Effects of early intensive blood pressure lowering treatment on the growth of hematoma and perihematomal edema in acute intracerebral hemorrhage: the Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial (INTERACT) Stroke. 2010;41:307–12. - PubMed
-
- Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med. 2013;368:2355–65. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical