

Systemic therapy in metastatic renal cell carcinoma
- PMID: 27277600
- PMCID: PMC5272893
- DOI: 10.1007/s00345-016-1868-5
Systemic therapy in metastatic renal cell carcinoma
Abstract
Purpose: Current systemic treatment of targeted therapies, namely the vascular endothelial growth factor-antibody (VEGF-AB), VEGF receptor tyrosine kinase inhibitor (TKI) and mammalian target of rapamycin (mTOR) inhibitors, have improved progression-free survival and replaced non-specific immunotherapy with cytokines in metastatic renal cell carcinoma (mRCC).
Methods: A panel of experts convened to review currently available phase 3 data for mRCC treatment of approved agents, in addition to available EAU guideline data for a collaborative review as the plurality of substances offers different options of first-, second- and third-line treatment with potential sequencing.
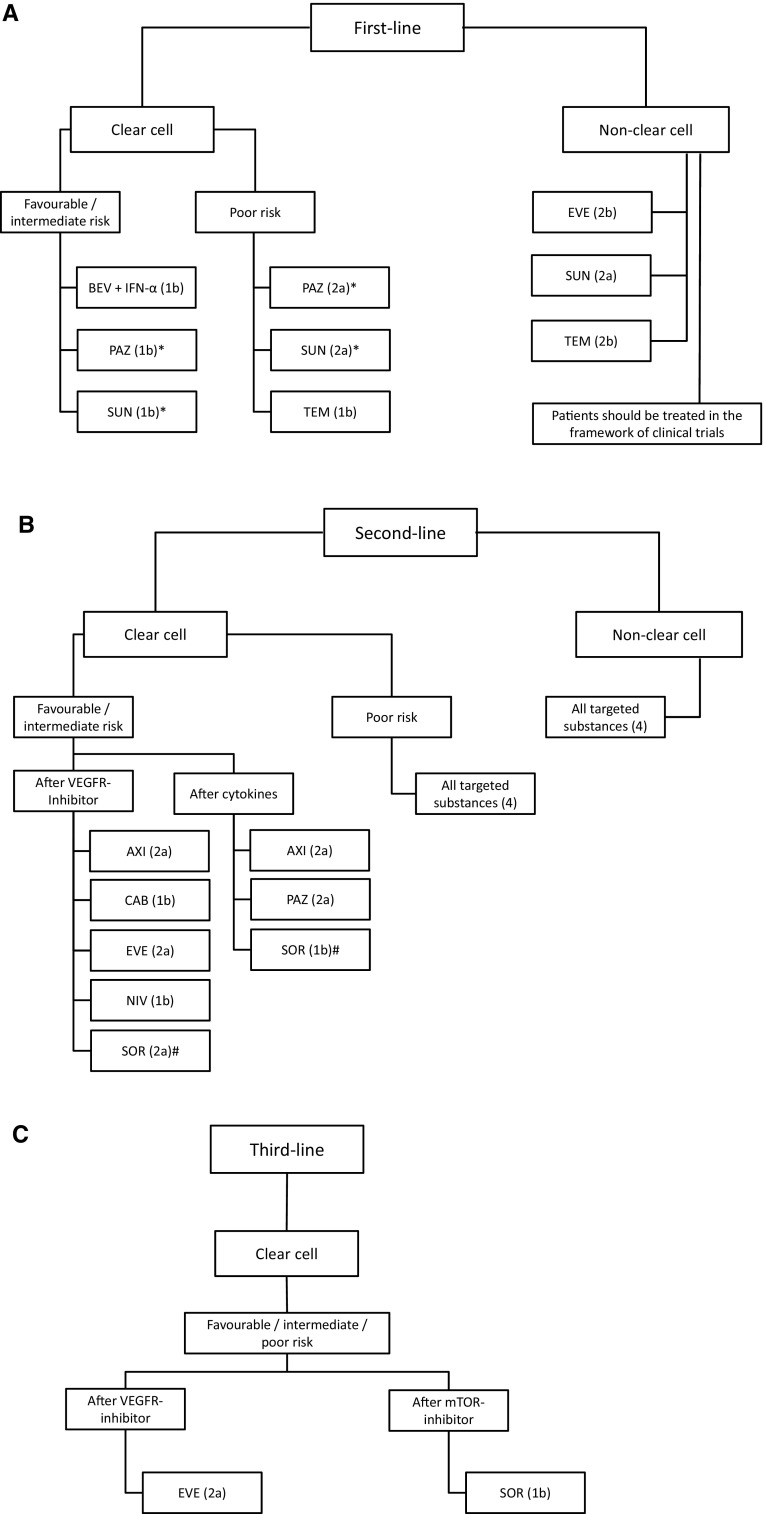
Results: Sunitinib and pazopanib are approved treatments in first-line therapy for patients with favorable- or intermediate-risk clear cell RCC (ccRCC). Temsirolimus has proven benefit over interferon-alfa (IFN-α) in patients with non-clear cell RCC (non-ccRCC). In the second-line treatment TKIs or mTOR inhibitors are treatment choices. Therapy options after TKI failure consist of everolimus and axitinib. Available third-line options consist of everolimus and sorafenib. Recently, nivolumab, a programmed death-1 (PD1) checkpoint inhibitor, improved overall survival benefit compared to everolimus after failure of one or two VEGFR-targeted therapies, which is likely to become the first established checkpoint inhibitor in mRCC. Data for the sequencing of agents remain limited.
Conclusions: Despite the high level of evidence for first and second-line treatment in mRCC, data for third-line therapy are limited. Possible sequences include TKI-mTOR-TKI or TKI-TKI-mTOR with the upcoming checkpoint inhibitors in perspective, which might settle a new standard of care after previous TKI therapy.
Keywords: Checkpoint inhibitor; Renal cell carcinoma; Sequence; Systemic treatment; Targeted therapy; Tyrosine kinase inhibitor mTOR inhibition.
Conflict of interest statement
AH: consultancies, honoraria or study participation from Pierre Fabre, BMS, GSK and Novartis. JB: consultancies, honoraria or study participation from Bayer, BMS, GSK, Immatics, Novartis, Pfizer and Roche. EH: consultancies, honoraria or study participation from Bayer, BMS, GSK, Novartis and Pfizer. JJ: Consultancies and honoraria of study participation from: Roche, Pfizer, GSK, Bayer, Lilly, Janssen-Cilag, Amgen, Celgene, Sanofi, Pharma Mar, Puma, Teva, Merck Sereno, Novartis. MS: consultancies, honoraria or study participation from Bayer, BMS, Novartis and Roche. SH: consultancies, honoraria from Novartis. SS: consultancies, honoraria or study participation from Amgen, Janssen-Cilag, Celgene, Novartis und MSD Sharp & Dohme. TG: consultancies or honoraria: Bayer, BMS, GSK, Novartis, Roche. VG: consultancies, honoraria or travel support: Bayer, BMS; Novartis, Pfizer.
Figures

References
-
- Rohan SM, Xiao Y, Liang Y, Dudas ME, Al-Ahmadie HA, Fine SW, Gopalan A, Reuter VE, Rosenblum MK, Russo P, Tickoo SK. Clear-cell papillary renal cell carcinoma: molecular and immunohistochemical analysis with emphasis on the von Hippel-Lindau gene and hypoxia-inducible factor pathway-related proteins. Modern Pathol. 2011;24(9):1207–1220. doi: 10.1038/modpathol.2011.80. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
