

Anticoagulation and population risk of stroke and death in incident atrial fibrillation: a population-based cohort study
- PMID: 27280108
- PMCID: PMC4866920
- DOI: 10.9778/cmajo.20150096
Anticoagulation and population risk of stroke and death in incident atrial fibrillation: a population-based cohort study
Abstract
Background: Atrial fibrillation increases the risk of stroke and death. Anticoagulation therapy is an effective treatment for stroke prevention, but remains underused in the community. We sought to determine the effectiveness and safety of anticoagulation therapy in an inception cohort with new-onset atrial fibrillation in the province of Alberta, Canada.
Methods: We conducted a population-based cohort study of atrial fibrillation using an administrative database from Alberta's publicly funded and universally available health care system. All new-onset atrial fibrillation patients from Jan. 1, 2009, to Dec. 31, 2010, were included in the cohort and followed through Dec. 31, 2013. We assessed anticoagulation status as a predictor of stroke and death using time-to-event analysis and adjusted for sex and CHADS2 (congestive heart failure, hypertension, age ≥ 75 yr, diabetes mellitus and prior stroke or transient ischemic attack) score using Cox proportional hazards modelling.
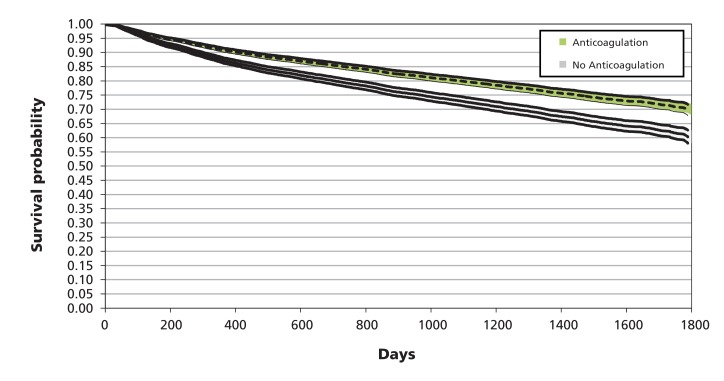
Results: We identified 10 745 patients, 7358 (68.5%) of whom received anticoagulation therapy, principally with warfarin (n = 6997, 95.1%). Anticoagulation therapy was associated with significantly decreased risk of ischemic stroke (hazard ratio [HR] 0.69, 95% confidence interval [CI] 0.58-0.82), all stroke (HR 0.77, 95% CI 0.65-0.91), all stroke and death (HR 0.70, 95% CI 0.62-0.72) and all-cause mortality (HR 0.67, 95% CI 0.62-0.72), despite an association with increased risk of hemorrhagic stroke (HR 1.92, 95% CI 1.17-3.16). There was a neutral association with subdural (HR 1.01, 95% CI 0.53-1.93) and gastrointestinal (HR 0.96, 95% CI 0.70-1.31) hemorrhage.
Interpretation: Anticoagulation therapy is effective and safe for stroke prevention and decreases mortality in patients with incident atrial fibrillation. These population data support an aggressive approach to screening for atrial fibrillation and treatment with anticoagulant medicines to prevent stroke and death.
Conflict of interest statement
Figures
References
-
- Lip GY, Tse HF. Management of atrial fibrillation. Lancet. 2007;370:604–18. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22:983–8. - PubMed
-
- Benjamin EJ, Wolf PA, D'Agostino RB, et al. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98:946–52. - PubMed
-
- Hart RG, Halperin JL, Pearce LA, et al. Lessons from the Stroke Prevention in Atrial Fibrillation trials. Ann Intern Med. 2003;138:831–8. - PubMed
-
- Andrew N, Kilkenny M, Harris D, et al. Outcomes for people with atrial fibrillation in an Australian national audit of stroke care. Int J Stroke. 2014;9:270–7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials