

Preclinical Studies of Mesenchymal Stem Cell (MSC) Administration in Chronic Obstructive Pulmonary Disease (COPD): A Systematic Review and Meta-Analysis
- PMID: 27280283
- PMCID: PMC4900582
- DOI: 10.1371/journal.pone.0157099
Preclinical Studies of Mesenchymal Stem Cell (MSC) Administration in Chronic Obstructive Pulmonary Disease (COPD): A Systematic Review and Meta-Analysis
Abstract
Background: In the last two decades, mesenchymal stem cells (MSCs) have been pre-clinically utilized in the treatment of a variety of kinds of diseases including chronic obstructive pulmonary disease (COPD). The aim of the current study was to systematically review and conduct a meta-analysis on the published pre-clinical studies of MSC administration in the treatment of COPD in animal models.
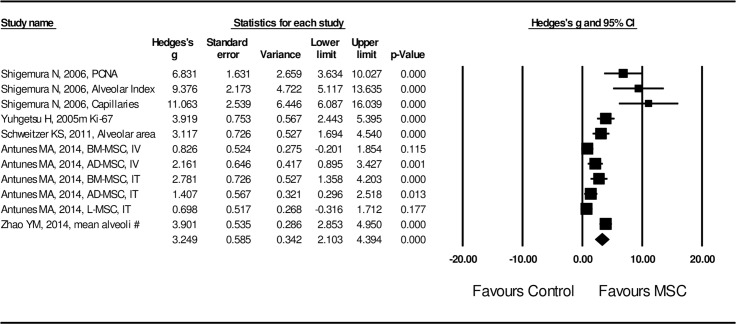
Methods and results: A systematic search of electronic databases was performed. Statistical analysis was performed using the Comprehensive Meta-Analysis software (Version 3). The pooled Hedges's g with 95% confidence intervals (95% CIs) was adopted to assess the effect size. Random effect model was used due to the heterogeneity between the studies. A total of 20 eligible studies were included in the current systematic review. The overall meta-analysis showed that MSC administration was significantly in favor of attenuating acute lung injury (Hedges's g = -2.325 ± 0.145 with 95% CI: -2.609 ~ -2.040, P < 0.001 for mean linear intercept, MLI; Hedges's g = -3.488 ± 0.504 with 95% CI: -4.476 ~ -2.501, P < 0.001 for TUNEL staining), stimulating lung tissue repair (Hedges's g = 3.249 ± 0.586 with 95% CI: 2.103~ 4.394, P < 0.001) and improving lung function (Hedges's g = 2.053 ± 0.408 with 95% CI: 1.253 ~ 2.854, P< 0.001). The mechanism of MSC therapy in COPD is through ameliorating airway inflammation (Hedges's g = -2.956 ± 0.371 with 95% CI: -3.683 ~ -2.229, P< 0.001) and stimulating cytokine synthesis that involves lung tissue repair (Hedges's g = 3.103 ± 0.734 with 95% CI: 1.664 ~ 4.541, P< 0.001).
Conclusion: This systematic review and meta-analysis suggest a promising role for MSCs in COPD treatment. Although the COPD models may not truly mimic COPD patients, these pre-clinical studies demonstrate that MSC hold promise in the treatment of chronic lung diseases including COPD. The mechanisms of MSCs role in preclinical COPD treatment may be associated with attenuating airway inflammation as well as stimulating lung tissue repair.
Conflict of interest statement
Figures






References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
