

Adequacy of Mental Health Services for HIV-Positive Patients with Depression: Ontario HIV Treatment Network Cohort Study
- PMID: 27280751
- PMCID: PMC4900603
- DOI: 10.1371/journal.pone.0156652
Adequacy of Mental Health Services for HIV-Positive Patients with Depression: Ontario HIV Treatment Network Cohort Study
Abstract
Background: Major depression can profoundly impact clinical and quality-of-life outcomes of people living with HIV, and this disease is underdiagnosed and undertreated in many HIV-positive individuals. Here, we describe the prevalence of publicly funded primary and secondary mental health service use and antidepressant use, as well as mental health care for depression in accordance with existing Canadian guidelines for HIV-positive patients with depression in Ontario, Canada.
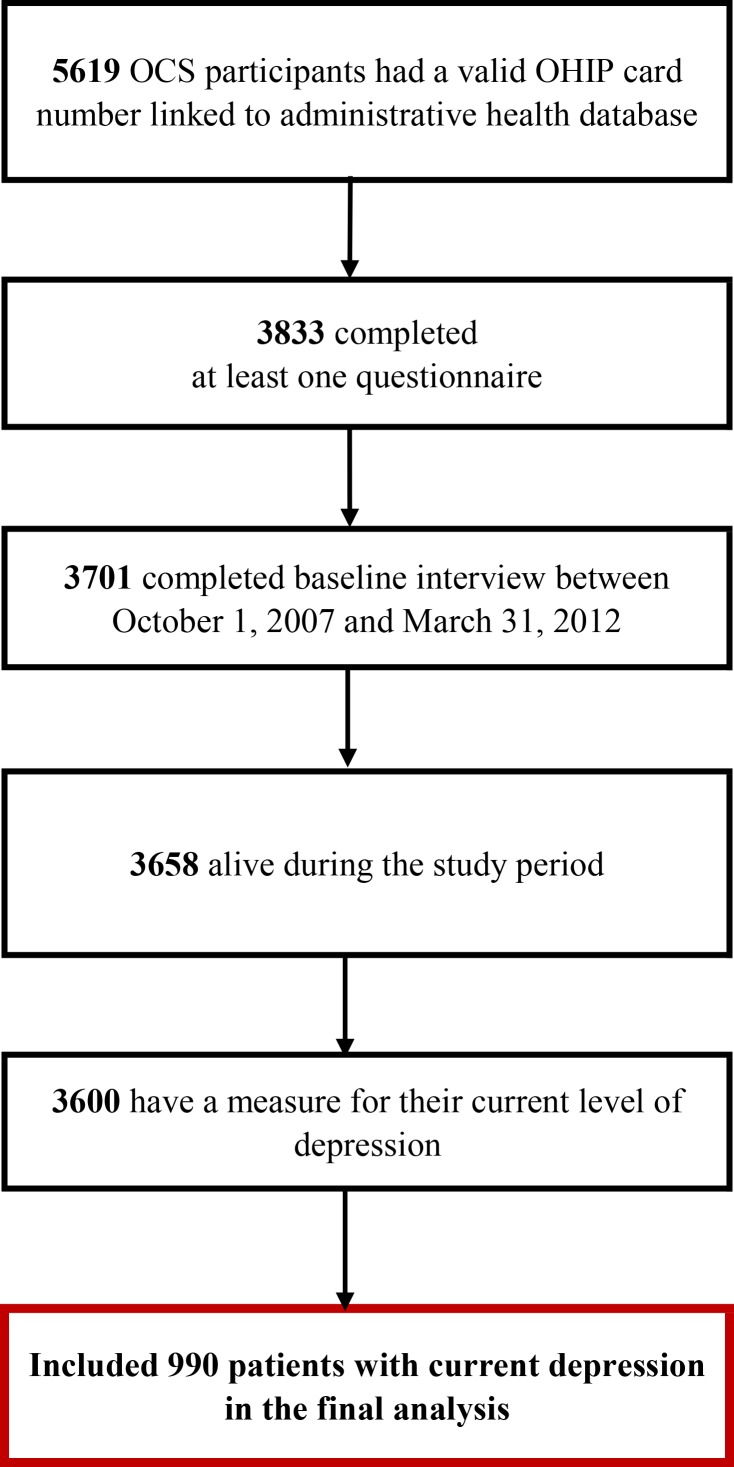
Methods: We conducted a prospective cohort study linking data from the Ontario HIV Treatment Network Cohort Study with administrative health databases in the province of Ontario, Canada. Current depression was assessed using the Center for Epidemiologic Depression Scale or the Kessler Psychological Distress Scale. Multivariable regressions were used to characterize prevalence outcomes.
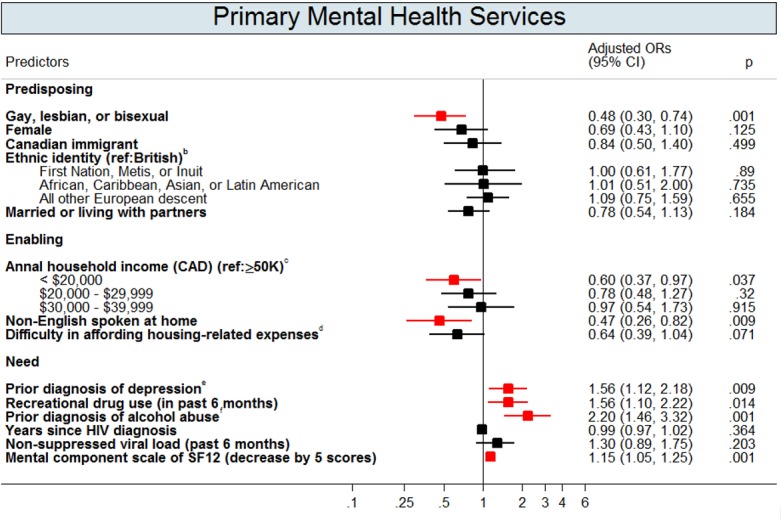
Results: Of 990 HIV-positive patients with depression, 493 (50%) patients used mental health services; 182 (18%) used primary services (general practitioners); 176 (18%) used secondary services (psychiatrists); and 135 (14%) used both. Antidepressants were used by 407 (39%) patients. Patients who identified as gay, lesbian, or bisexual, as having low income or educational attainment, or as non-native English speakers or immigrants to Canada were less likely to obtain care. Of 493 patients using mental health services, 250 (51%) received mental health care for depression in accordance with existing Canadian guidelines.
Conclusions: Our results showed gaps in delivering publicly funded mental health services to depressed HIV-positive patients and identified unequal access to these services, particularly among vulnerable groups. More effective mental health policies and better access to mental health services are required to address HIV-positive patient needs and reduce depression's impact on their lives.
Conflict of interest statement
Figures



References
-
- Katz MH, Douglas JMJ, Bolan GA, Marx R, Sweat M, Park M- SS, et al. Depression and use of mental health services among HIV-infected men. AIDS Care. 1996;8:433–42. - PubMed
-
- Taylor SL, Burnam AM, Sherbourne CD, Andersen R, Cunningham WE. The Relationship Between Type of Mental Health Provider and Met and Unmet Mental Health Needs in a Nationally Representative Sample of HIV-positive Patients. J. Behav. Health Serv. Res. 2004;31:149–63. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
